Table of Contents
Introduction
Imagine experiencing sudden, intense bursts of sharp, electric-like pain on one side of your face – that’s the reality for those living with trigeminal neuralgia. Curious to learn more about this condition and how it affects daily life? Keep reading to uncover the causes, symptoms, and treatments for this debilitating disorder.
So, what exactly is neuralgia?
Neuralgia” actually comes from two Greek words: “neuron” meaning nerve, and “algos” meaning pain. So, yeah, it basically means nerve pain. It’s that sharp, stabbing, or burning pain that travels along a nerve. It usually happens when the nerve gets irritated, damaged, or inflamed. The pain can feel different depending on how bad it is, and things like touch, movement, or even certain triggers can set it off.

What is the trigeminal nerve?
- The trigeminal nerve is the largest cranial nerve and is responsible for the sensory supply of the face and the motor and sensory supply to the muscles of mastication.
- The trigeminal nerve has peripheral (located outside the brain and spinal cord) sensory components converging at the trigeminal ganglia that relay touch, pain, and temperature information from the ipsilateral (on the same side of the body) face to the contralateral thalamus (sensory and motor signals from one side of the body are often processed by the thalamus on the opposite side of the brain) via the trigeminothalamic tract [1]
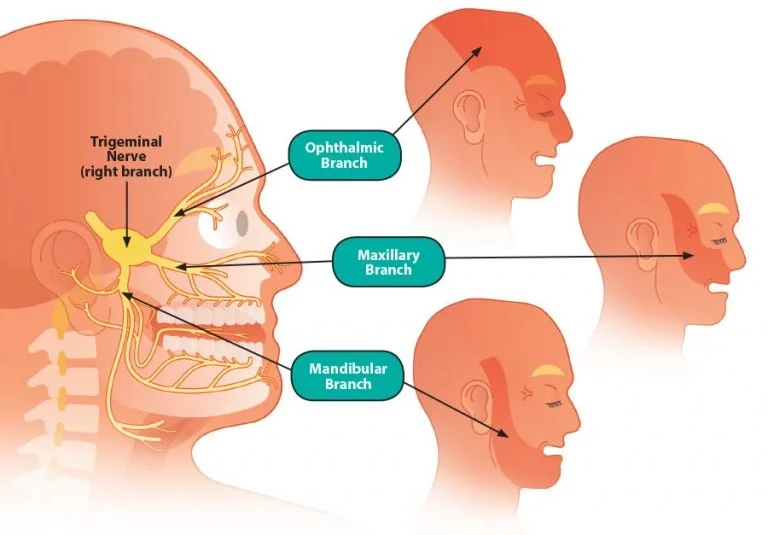
The trigeminal nerve has 3 divisions: ophthalmic (V1), maxillary (V2), and mandibular (V3). The anatomical areas innervated by each division are as follows:
- Ophthalmic (V1): eye, upper eyelid, and forehead
- Maxillary (V2): lower eyelid, cheek, nostril, upper lip, and upper gingivae
- Mandibular (V3): lower lip, lower gingivae, jaw, and the muscles of mastication.
What is trigeminal neuralgia?
- Trigeminal neuralgia is a condition characterised by pain coming from the trigeminal nerve, which starts near the top of the ear and splits in three, toward the eye, cheek, and jaw. We have two trigeminal nerves, one for each side of our face, but trigeminal neuralgia pain most commonly affects only one side.
- Pain along the trigeminal nerve, which affects the face.
- Pain is sudden,
- usually unilateral (pain typically affects one side of the face (not both sides)),
- severe,
- brief (pain doesn’t last long; it comes and goes quickly.),
- stabbing (pain feels like being poked or stabbed with something sharp), lancinating (this just means the pain shoots or spreads along a specific path, like a sudden electric shock),
- paroxysmal (pain comes in episodes or attacks, often with no clear cause or trigger),
- recurring pain (pain can come back over time, with breaks in between) in the distribution of one or more branches of the 5th cranial nerve.
- It is a truly agonizing condition in which patient may clutch the hand over the face and experience severe, lancinating pain associated with spasmodic contractions of the facial muscles during attacks—a feature that led to the use of the term (its archaic name) “Tic Douloureux” (painful jerking)
Summary
Location and Unilateral Pain: Trigeminal neuralgia causes pain along the trigeminal nerve, usually on one side of the face, affecting areas like the eye, cheek, and jaw.
Sharp and Sudden Pain: The pain is sudden, severe, stabbing, and brief, often described as an electric shock-like sensation that occurs in episodes.
Recurring and Agonizing Attacks: The condition leads to recurring episodes of pain, often with facial muscle spasms, causing intense discomfort, which is why it’s sometimes referred to as “Tic Douloureux”.
Trigeminal neuralgia causes
- There are two types of TN—primary and secondary.
- The exact cause of TN is still unknown, but the pain associated with it represents an irritation of the nerve.
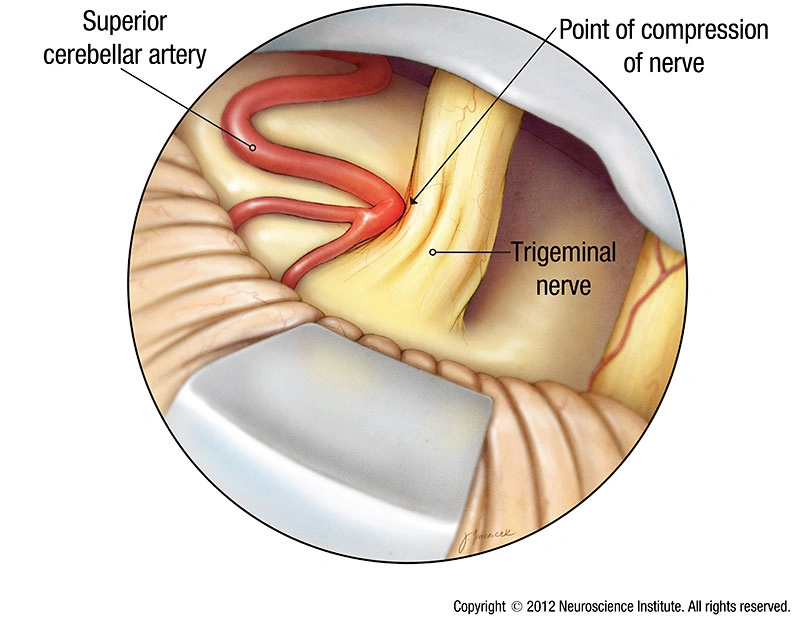
- Primary trigeminal neuralgia has been linked to the compression of the nerve, typically in the base of the head where the brain meets the spinal cord.
- This is usually due to contact between a healthy artery or vein and the trigeminal nerve at the base of the brain.
- This places pressure on the nerve as it enters the brain and causes the nerve to misfire.
- Secondary trigeminal neuralgia is caused by pressure on the nerve from a tumor, MS, a cyst, facial injury or another medical condition that damages the myelin sheaths, i.e Multiple sclerosis
Summary
Primary Trigeminal Neuralgia: Caused by nerve compression at the brainstem due to contact between an artery or vein and the trigeminal nerve.
Secondary Trigeminal Neuralgia: Triggered by pressure on the nerve from conditions like tumors, cysts, or diseases like multiple sclerosis.
Unknown Cause: The exact cause is unclear, but pain results from irritation or pressure on the trigeminal nerve.
Trigeminal neuralgia trigger points
Several triggers may set off the pain of trigeminal neuralgia, including:
- Shaving.
- Touching your face.
- Eating.
- Drinking.
- Brushing your teeth.
- Talking.
- Putting on makeup.
- A light breeze blowing over your face.
- Smiling.
- Washing your face.
What is the mechanism of the disease?
- Most cases of trigeminal neuralgia are due to trigeminal nerve compression and subsequent nerve demyelination in the area of compression.
- How demyelination leads to the symptoms of trigeminal neuralgia is unknown. It is hypothesized that ectopic impulse generation induced by the demyelinated lesion causes ephaptic transmission, defined as electrical conduction between adjacent neurons through extracellular spaces without using synapses or neurotransmitters.[2]
- Therefore, the drastic increase in posttrigger neuronal activity recruits additional neighbouring neurones, leading to a rapid accumulation of electrical activity, which can be amplified by ephaptic interaction among neurones, since the myelin sheath is damaged and nerve fibers maintain close contact among them.[3]
- The bioresonance hypothesis states that when the vibration frequency of the trigeminal nerve and surrounding structures approach one another, the trigeminal nerve fibers are damaged, leading to abnormal transmission of impulses, resulting in facial pain.[4]
Trigeminal neuralgia symptoms
- Pain may be like stabbing, electric shocks, burning, pressing, crushing, exploding, shooting, boring, shock-like sensations, migraine-like, piercing, prickling, or a combination.[5]
- Usually, pain resolves completely between the attacks. It usually does not occur when the person is asleep. It is estimated that 1 in 15,000 or 20,000 people suffer from TN; the actual figure may be higher due to frequent misdiagnosis. [6]
- During an attack, the patient grimaces with pain, clutches his hands over the affected side of the face, stopping all the activities, and holds or rubs his face, which may redden or the eyes water until the attack subsides. Male patients avoid shaving. The oral hygiene is poor, as the patient avoids brushing of teeth.
- Disease usually involves a single division; it may slowly spread to other divisions. TN may be associated with ipsilateral hemifacial spasm (painful tic convulsive).[7]
- Many patients will lead a very poor quality of life because of excruciating pain.
- It is usually unilateral; bilateral presentation is rare. [8]
- Rapid spreading to other division, bilateral involvement, or simultaneous involvement of other nerve suggests a secondary disease such as multiple sclerosis (MS) or an expanding cranial tumor. [9]
- It is common after 50 years of age. TN is uncommon in young adults. Presentation in children is rare. It is more common in females than males [10]
- The paroxysms occur in cycles, each cycle lasting for weeks or months, and with time, the cycle appears closer and closer. With each attack, the pain seems to become more intense and unbearable.
- It is very common for these patients to undergo indiscriminate dental extractions on the affected side without any relief from pain because the pain of the trigger zone and pain fiber distributions often mimic pain of odontogenic origin.
Trigeminal neuralgia diagnosis
- The White and Sweet criteria were incorporated into the official research by the International Association for the Study of Pain—IASP and the International Headache Society—IHS. The current IHS recommended classification for TN is listed in “International Classification of Headache Disorders II—ICHD-II
- Sweet diagnostic 5 major criteria for trigeminal neuralgia
- The pain is paroxysmal
- The pain may be provoked by light touch to the face (trigger zones).
- The pain is confined to the trigeminal distribution.
- The pain is unilateral
- The clinical sensory examination is normal
ICHD-III Diagnostic Criteria for Classical TN:
- A. At least one of the following characteristics:
- Paroxysms of severe, stabbing, electric shock-like pain in the distribution of one or more branches of the trigeminal nerve, typically involving V2 (maxillary) and V3 (mandibular) branches, but it may involve V1 (ophthalmic).
- Pain attacks are unilateral (on one side of the face).
- The pain lasts for a few seconds to a couple of minutes.
- Pain is triggered by mild stimuli such as touch, chewing, brushing teeth, or wind.
- B. There is no evidence of any other cause for the pain (i.e., the pain is not secondary to a structural lesion or any neurological disease like multiple sclerosis).
- C. Between attacks, the patient is pain-free, without any residual discomfort.
- D. The patient has no other neurological abnormalities between the attacks.
ICHD-III Diagnostic Criteria for Symptomatic TN:
- A. At least one of the following characteristics:
- Paroxysms of severe, stabbing, electric shock-like pain in the distribution of one or more branches of the trigeminal nerve (usually unilateral, but may occasionally be bilateral).
- Pain lasts seconds to a couple of minutes.
- Pain is triggered by mild stimuli like touch, wind, or chewing.
- B. A structural lesion is identified by imaging (MRI) or another diagnostic method, such as a tumor, multiple sclerosis, vascular malformation, or another pathological process, which directly affects the trigeminal nerve or its root.
- C. Between pain attacks, the patient may experience persistent discomfort or a dull ache, in contrast to the complete pain-free intervals typically seen in classical TN.
Key Differences Between Classical and Symptomatic TN in ICHD-III:
- Classical TN is typically idiopathic, often caused by vascular compression of the trigeminal nerve without any underlying neurological disease. It is the most common form of TN.
- Symptomatic TN is secondary to a neurological disorder or structural lesion, like multiple sclerosis or a tumor, and may be bilateral in some cases (especially in multiple sclerosis).
trigeminal neuralgia MRI
Patients with a clinical diagnosis of trigeminal neuralgia should undergo neuroimaging with magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) whenever possible. MRI is preferable to computed tomography. [11]
Detection of changes in trigeminal root
Atrophic changes are also associated in TN. Coregistration of three-dimensional fast imaging employing steady-state (3D FIESTA) imaging and DTI facilitates excellent delineation of cisternal segments of TR Ns[12]
Trigeminal neuralgia treatment
Trigeminal neuralgia drugs
- The antiepileptics carbamazepine or oxcarbazepine are the preferred initial therapeutic agents; only carbamazepine is approved by the United States Food and Drug Administration (FDA) for treating trigeminal neuralgia. These antiepileptic agents may control pain by binding to voltage-gated sodium channels. [11]
- Both medications are initiated at a low dose and titrated upward until the pain is controlled. Neither medication provides immediate relief; assessments of therapy must not occur before 2 weeks after initiation.[13]
- These medications control pain for most people, perhaps 70%, in the early stages of the disease. In some patients, the effectiveness of carbamazepine decreases over time [14]
- Carbamazepine 100 mg three times a day is introduced and titrated over 1–5 weeks period until either remission is achieved or side effects or toxicity are unacceptable. (Commercially, tegretol 100 mg, 200 mg or 400 mg tablets are available. Controlled or slow release tablets are available).
- The dosage of the drug used initially should be kept small to minimum, especially in elderly patients to avoid nausea, vomiting and gastric irritation. More of daily drug dosage should be taken at night, so that adequate serum concentration can be present in early morning, when pain most occurs. Complete blood count with platelet count, liver function screening should be done prior to treatment, a month after treatment and at 3–4 months intervals, particularly, if patient continues to receive a high dose (1,000–1,500 mg/day).
- Adverse effects of carbamazepine include drowsiness, dizziness, diplopia, and nausea. In patients of Asian ancestry, before starting carbamazepine, testing for the HLA-B*15:02 allele is recommended; this allele is strongly associated with developing toxic epidermal necrolysis or Stevens-Johnson syndrome when taking carbamazepine and structurally related pharmaceuticals [15] Oxcarbazepine is a newer drug increasingly used as first-line therapy for patients with trigeminal neuralgia who do not respond to or tolerate carbamazepine; oxcarbazepine should also be avoided in those testing positive for the HLA-B*15:02 allele.
Trigeminal neuralgia operation
- Surgical intervention is recommended for patients with classic trigeminal neuralgia who have failed maximal medical therapy. Some interventions include microvascular decompression, rhizotomy, and peripheral nerve block. These methods have varying levels of initial efficacy and pain recurrence rates. [13]
Microvascular decompression
- Microvascular decompression is one of the most frequently employed procedures to treat trigeminal neuralgia and benefits patients with compression of the nerve root. [16]
- Microvascular decompression is performed via craniotomy and posterior fossa exploration to identify and relocate the compressing blood vessel. A soft cushion is placed between the nerve and the offending vessel to allow the nerve to recover and the pain to abate. The procedure is efficacious in greater than 90% of patients; pain recurs in approximately 10%, usually within the 2 years following the procedure. [13]
- Microvascular decompression is an invasive procedure with the associated complications of partial hearing loss, cerebellar hematoma, cerebrospinal fluid leaks, infarction, and facial weakness. However, microvascular decompression is currently the most effective long-term surgical treatment available to patients with trigeminal neuralgia.[17]
Rhizotomy
- Microvascular ablative procedures include rhizotomy with thermocoagulation, chemical injection, or mechanical balloon compression to damage the trigeminal nerve root and interrupt pain signal transmission. Rhizotomy with thermocoagulation employs heat via an electrode, chemical rhizotomy injects glycerol directly into the trigeminal nerve, and balloon compression mechanically damages nerve fibers. The result of rhizotomy is decreased signal transmission [18], [19]
- Complications of rhizotomy include postoperative dysesthesia, corneal numbness, sensory loss in trigeminal nerve distribution, and anesthesia dolorosa, or numbness and spontaneous pain without stimuli. [20]
Stereotactic Radiosurgery
- The use of radiotherapy in trigeminal neuralgia may be considered in patients who have failed maximal medical therapy, are poor surgical candidates, or have failed surgical intervention. Radiotherapy is a noninvasive procedure wherein a highly concentrated dose of ionizing radiation is delivered to a precise target at the trigeminal nerve root. The radiation creates a lesion near the nerve root, interrupting the pain signals from transmission to the brain. Lesion formation is slow, and hence, the pain relief offered by this procedure is delayed by several weeks or months.
- trigeminal neuralgia gamma knife – Gamma Knife®, a cobalt-60 source-based system, has been used extensively and has the largest recorded data set regarding outcomes in patients with trigeminal neuralgia.[21]
- Alternative delivery systems include linear accelerator-based (Single-treatment stereotactic radiosurgery ) SRS (LINAC) and robotic radiosurgery with CyberKnife®. The treatment outcomes appear comparable between all 3 systems [21]
Simulation
- In a conventional Gamma Knife® system, a rigid stereotactic headframe immobilization system is fixed directly to the patient’s skull. However, there are reports of “frameless” stereotactic radiosurgery employing thermoplastic masks. LINAC-based SRS and Cyberknife® typically use a specialized thermoplastic facial mask. [22], [23]
Dosing
Doses range from 70 to 90 Gy delivered in a single session; 70 Gy is considered the minimal effective dose and 90 Gy the maximally effective dose. Efficacy is thought to be similar within that dose range, but the rate of complications tends to increase with dose escalation. The dose is prescribed to the 100% isodose line in Gamma Knife® cases, while LINAC-based SRS or CyberKnife® systems are typically prescribed to the 80% to 90% isodose lines
FAQs
Can trigeminal neuralgia be cured?
Trigeminal neuralgia does not have a permanent cure, but there are effective treatments available to manage the condition. Medications like anticonvulsants (e.g., carbamazepine) are often used to control the pain. For those who don’t respond to medications, surgical options, such as microvascular decompression or rhizotomy, may offer relief.
Trigeminal neuralgia natural treatment?
- Capsaicin: Applied topically, capsaicin cream can help reduce pain by desensitizing nerve endings.
- Turmeric (Curcumin): Known for its anti-inflammatory properties, turmeric may help reduce nerve inflammation.
- Ginger: Ginger can help with pain relief due to its anti-inflammatory and analgesic properties.
- Essential Oils: Oils like lavender and peppermint have been used in aromatherapy for pain relief and relaxation.
trigeminal neuralgia and dental pain
Trigeminal neuralgia (TN) and dental pain can both cause sharp facial pain, but they are different. TN results from nerve irritation and causes sudden, electric shock-like pain, often triggered by activities like chewing or talking. Dental pain is usually linked to issues like tooth decay or gum disease and tends to be more persistent. If the pain comes and goes suddenly without clear dental cause, it could be TN, so it’s important to seek a proper diagnosis.
can trigeminal neuralgia go away?
Trigeminal neuralgia (TN) is generally considered a chronic condition, and in most cases, it doesn’t completely “go away” on its own.
trigeminal neuralgia location
Trigeminal neuralgia (TN) typically causes severe, stabbing pain along the trigeminal nerve‘s path.



