The Ultimate Guide to Acute Necrotising Ulcerative Gingivitis
Table of Contents
Introduction
Acute Necrotising Ulcerative Gingivitis (ANUG) is a destructive (ulcerative + necrotizing) disease of the gums with various names such as Vincent’s infection and trench mouth. It is primarily seen in smokers and debilitated patients under stress, with poor oral hygiene and other factors contributing to its development. ANUG presents with crater-like lesions and can lead to rapid tissue destruction if left untreated. Treatment is tailored to the individual case.
Trench mouth: as it has shape of a trench or crater
Plaut-vincent stomatitis
Field stomatitis- due to very foetid odour= halitosis
What is ANUG?
Acute necrotizing ulcerative gingivitis is a painful infection that affects the gums primarily. ANUG occurs in people who are frequent smokers and debilitated patients who are under stress. Other factors that may cause ANUG are poor oral hygiene, nutritional deficiencies, immunodeficiency (e.g., HIV/AIDS, use of immunosuppressive drugs), and sleep deprivation. Some people can have oral candidiasis. ANUG is a rapidly destructive, non-communicable microbial disease of the gingiva in the context of an impaired host immune response.
History
NUG is characterized by its sudden onset, sometimes after an episode of debilitating disease or acute respiratory tract infection. A change in living habits, protracted work without adequate rest, poor nutrition, tobacco use, and psychological stress are frequent features of the patient’s history.
Oral Signs And Symptoms
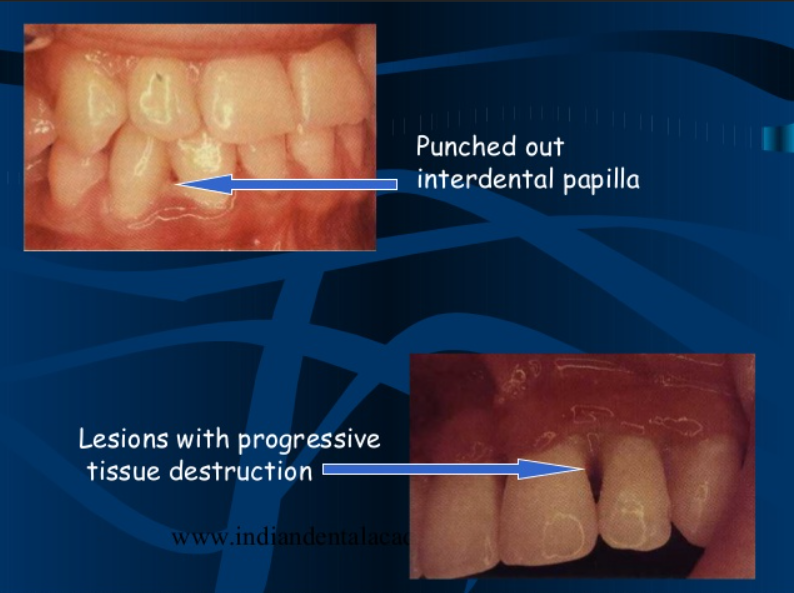
Characteristic lesions are punched-out, craterlike depressions at the crest of the interdental papillae that subsequently extend to the marginal gingiva and rarely to the attached gingiva and oral mucosa.
The surface of the gingival craters is covered by a gray, pseudomembranous slough that is demarcated from the remainder of the gingival mucosa by a pronounced linear erythema.
Spontaneous gingival hemorrhage or pronounced bleeding after the slightest stimulation are additional characteristic clinical signs.
The lesions are extremely sensitive to touch.In some cases, the lesions are denuded of the surface pseudomembrane, thereby exposing the gingival margin, which is red, shiny, and hemorrhagic. The characteristic lesions may progressively destroy the gingiva and the underlying periodontal tissues.
the patient often complains of a constant radiating, gnawing pain that is intensified by eating spicy or hot foods and chewing.
There is a “metallic” foul taste, and the patient is conscious of an excessive amount of “pasty” saliva.
Systemic Signs and Symptoms.
Patients are usually ambulatory and have a minimum of systemic symptoms.
Local lymphadenopathy and a slight elevation in temperature are common features of the mild and moderate stages of the disease.
In severe cases, there may be high fever, increased pulse rate, leukocytosis, loss of appetite, and general lassitude.
Systemic reactions are more severe in children. Insomnia, constipation, gastrointestinal disorders, headaches, and mental depression sometimes accompany the condition.
Bacteriology
The surface of the necrotic lesion contains microorganisms that morphologically resemble cocci, fusiform bacilli, and spirochetes.
Treponema microdentium. They occur in non-necrotic tissue before other types of bacteria, and they may be present in high concentrations intercellularly in the epithelium adjacent to the ulcerated lesion and in the connective tissue.
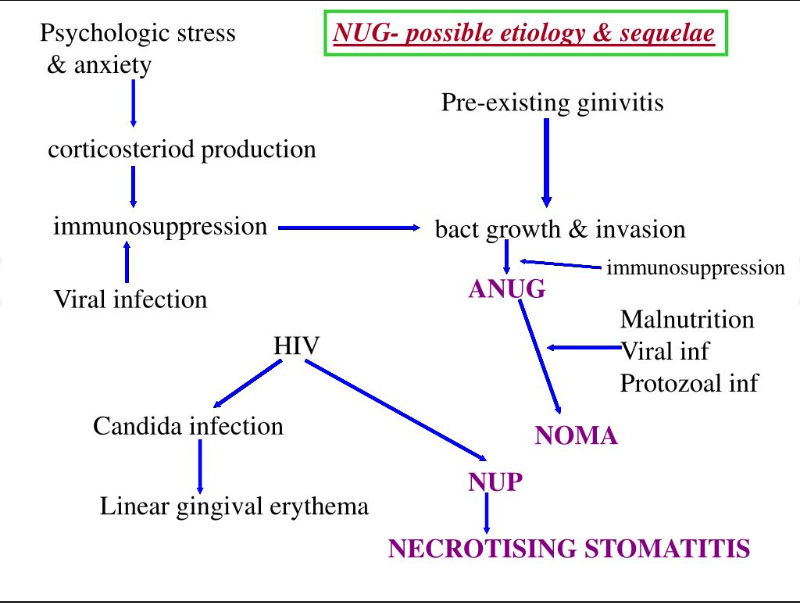
Etiology
The role of bacteria:
Opinion still differ regarding bacteria being primary causative factor of NUG
The specific cause of ANUG has not been established. But the prevalent opinion is that it is produced by a complex of bacterial organisms but requires underlying tissue changes to facilitate the pathogenic activity and effect of the bacteria. (predisposing factor).
Local predisposing factor:
Preexsisting chronic gingivitis or periodontal pockets or periocoronitis ( which are incubation zones because it’s favourable environment for activity and proliferation of MOs)
Areas of traumatised gingiva such as malocclusion decrease resistance of gingival tissue.
Smoking: smoking affects physiologic, immunologic and inflammatory response of the gingiva
Tobacco has a direct toxic effect on gingiva.
Nicotine affects the micro-vasculature of the gingiva by inducing production of noradrenaline leading to vasoconstriction.
Decreased O2 concentration in the gingival tissue leading to decrease of the oxidative killing mechanism of neutrophil and increase of anaerobic bacteria.
Decrease gingival crevicular fluid, gingival blood vessels and bleeding on probing.
Decrese neutrophil chemotaxis, phagocytosis and the oxidative killing mechanism.
Elevated levels of PGE and TNFa- causing bone resorption.
Smokers have a higher Ca+2 concentration in dental plaque than non smokers. This might influence the rate of calculus formation and contributes to further deterioration of oral hygiene- increasing subgingival calculus.
Systemic predisposing factors:
Nutritional deficiencies- e.g. vitamin C, vitamin B complex.
Debilitating disease- metallic intoxication, cachexia, severe GIT disorders, blood disease as leukemia, AIDS.
Psychosomatic factors- emotional stress.
Emotional stress: cause elevation of corticosteroid and catecholamine level which-
Good media for nutrition of P. intermedia (cortisol)
Alter gingival micro-vasculature. (decrease o2)
Decrease neutrophil chemotaxis and phagocytosis.
Decrease lymphocytic mitogen (mitosis) response.
Alter helper-suppressor lymphocyte ratio (CD4 & CD8) to facilitate bacterial invasion.
Diagnosis
Diagnosis is based on clinical findings of gingival pain, ulceration, and bleeding. A bacterial smear is not necessary or definitive, because the bacterial picture is not appreciably.
The microscopic examination of a biopsy specimen is not sufficiently specific to be diagnostic. It can be used to differentiate NUG from specific infections (e.g., tuberculosis) or from neoplastic disease, but it does not differentiate between NUG and other necrotizing conditions of nonspecific origin, such as those produced by trauma or caustic medications.
Zones of ANUG Tissues
The mechanisms by which the damage occurs to gingival tissues is not completely clear, however four zones have been identified in the gingival tissues:
Bacterial zone (the only zone found in situations aside from ANUG)
Neutrophil-rich zone
Necrotic zone
Spirochaetal infiltration zone
Damage occurs through direct toxic effects and indirect effects. Predisposing factors are also important in leading to ANUG in patients.
Clinical course
Stage 1- necrosis of the tip of the interdental papilla (93%) (NUG).
Stage 2– necrosis of the entire papilla (19%) (may be NUG or NUP depends on attachment loss).
Stage 3– necrosis extending to the gingival margin (21%) (NUP).
Stage 4- necrosis extending also to the attached gingiva (1%) (NUP).
Stage 5– necrosis extending into buccal or labial mucosa (6%) (necrotising stomatitis).
Stage 6– necrosis exposing alveolar bone (1%) (necrotizing stomatitis).
Differentiation Between Necrotizing Ulcerative Gingivitis and Primary Herpetic Gingivostomatitis
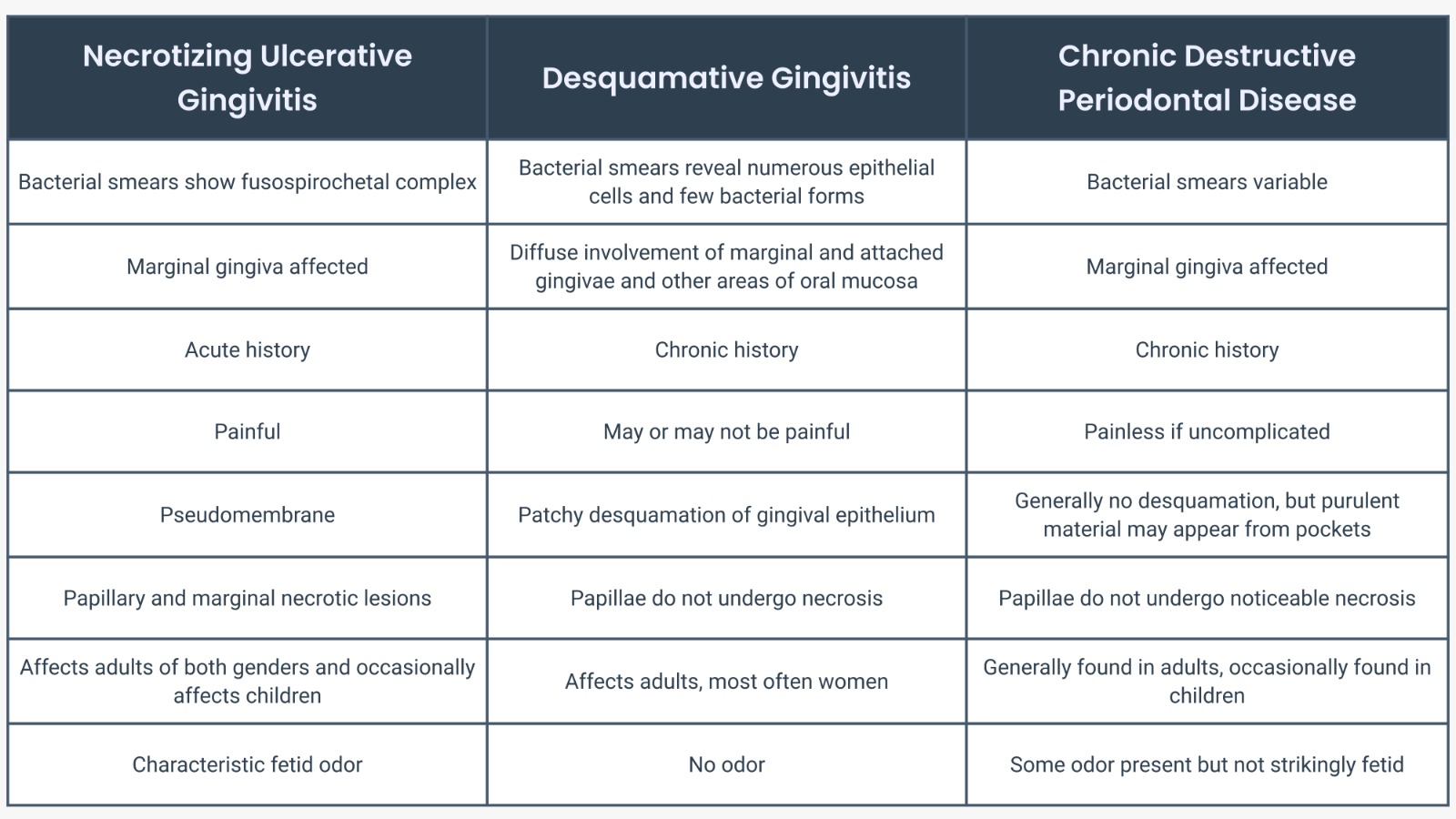
Differentiation Among Necrotizing Ulcerative Gingivitis, Chronic Desquamative Gingivitis, and Chronic Periodontal Disease
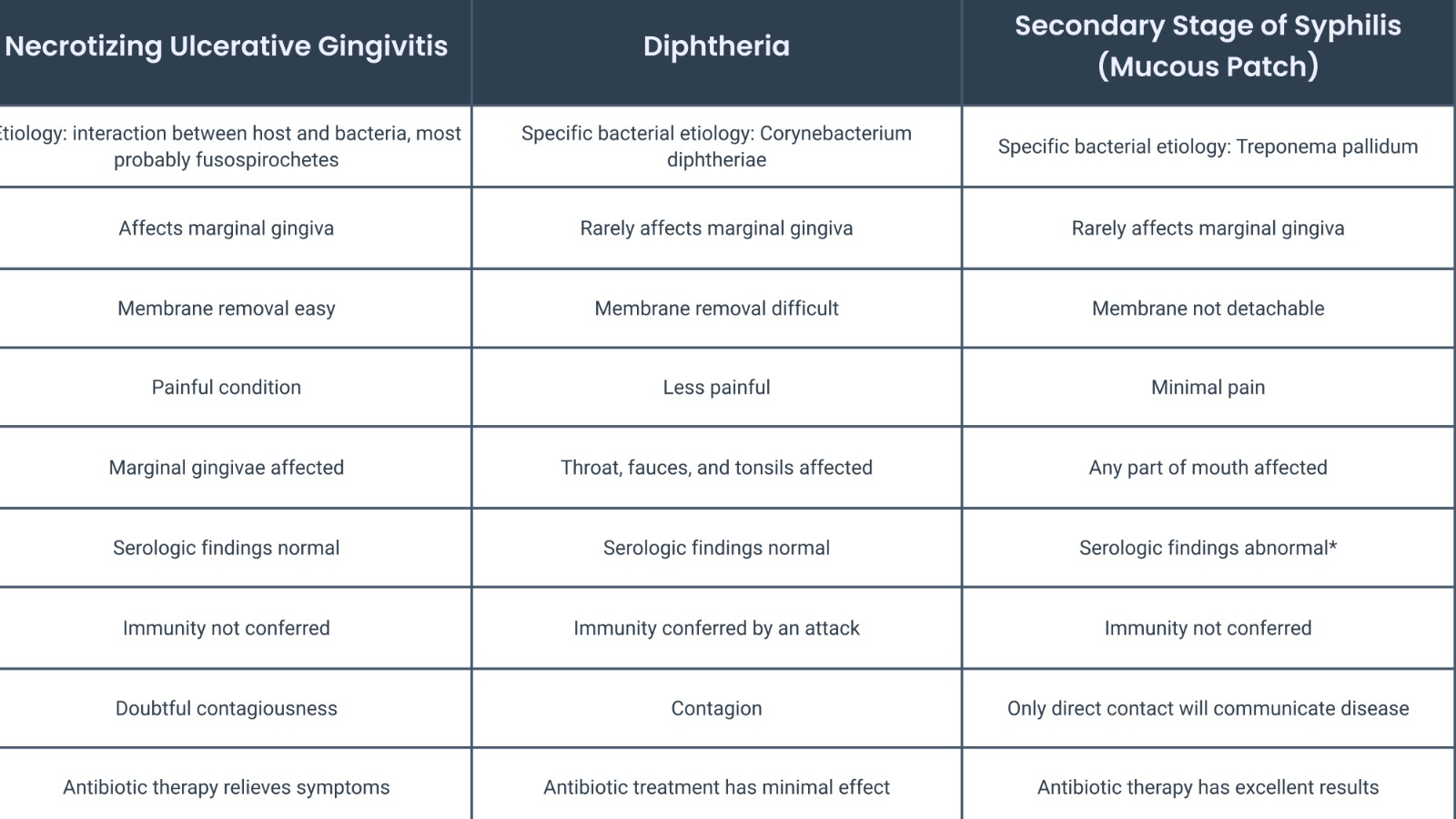
Differentiation Among Necrotizing Ulcerative Gingivitis, Diphtheria, and Secondary Stage of Syphilis
Predisposing Factors
There are multiple predisposing factors that are helpful to look out for in a patient who presents with potential ANUG:
Immune suppression – particularly patients with HIV infection (it may even be the first symptom presentation of someone with unknown HIV diagnosis)
Stress
Smoking
Poor diet or malnutrition
Pre-existing gingival conditions and poor oral hygiene
ANUG is more common in developing countries, often in children and where there is a high incidence of malnutrition or infections.
Treatment
Local: treat the acute inflammation & underlying cause (local predisposing factors).
Systemic:
a) supportive treatment: analgesic, bed rest, good nutrition, fluid intake, etc.
b) etiotropic treatment: TTT of systemic background.
Treatment should follow orderly sequences, so at the first visit:
General impression of the pt. background (recent illness, living conditions, dietary background, mental stress, social activity and distress, family and friend relations, his attitude, etc).
Patient general appearances (such as temperature & examination of lymph nodes to detect enlarged ones).
Examination of the oral cavity to examine the characteristic lesion & oral hygiene is evaluated.
Taking history disease (recurrent on for the first time).
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
DisagreeAgree
Connect with
I allow to create an account
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
DisagreeAgree
0 Comments
Oldest
NewestMost Voted
Inline Feedbacks
View all comments
Written By
Dr. Bharat Bhushan(BDS)
Dr. Bharat Bhushan is an India-based board-certified general dentist.