
Table of Contents
Introduction
Syncope: More Than Just a Fainting Spell! Discover the critical steps for emergency response, effective management, and proven treatments to handle syncope like a pro. Your guide to saving lives starts here!
Investigations and Diagnosis
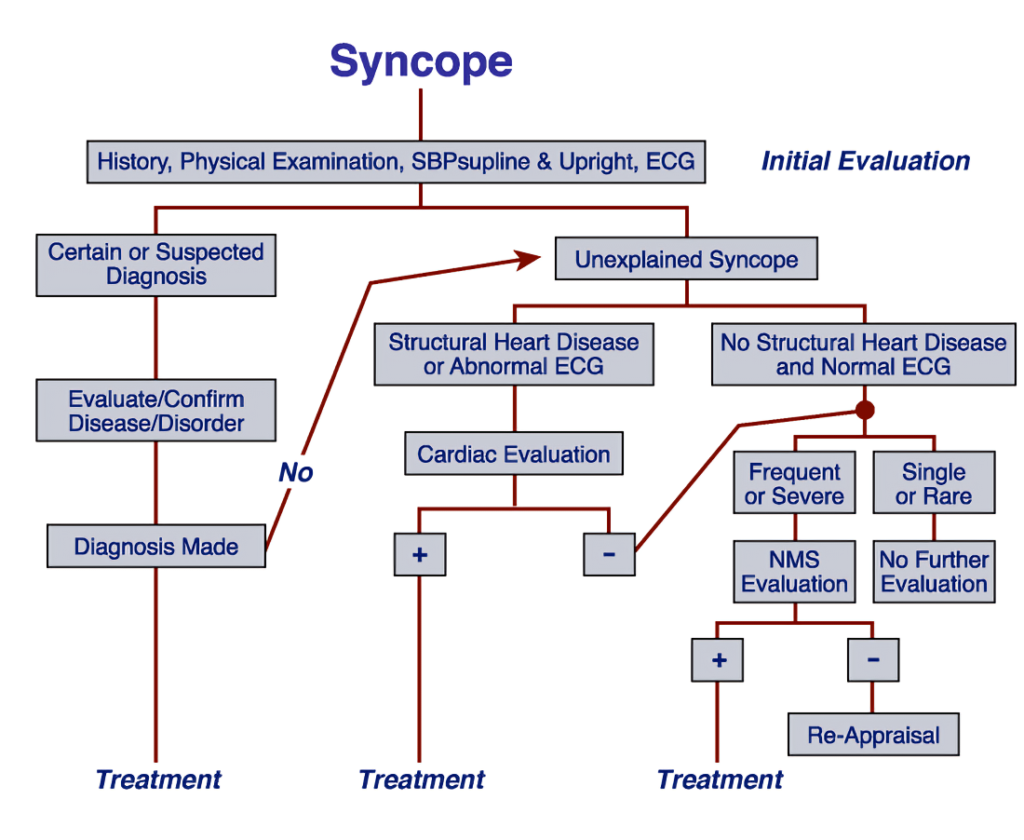
Initial Assessment:
- Syncope, commonly known as fainting, can be a sign of an underlying health issue and requires careful management. The process starts with a thorough evaluation by a healthcare professional, which includes:
- Medical History Review:
- The doctor will ask about the frequency, duration, and triggers of your fainting episodes (e.g., standing up quickly, emotional stress).
- They’ll also note any associated symptoms, such as lightheadedness, palpitations, or nausea.
- Physical Examination:
- A detailed check-up focusing on your cardiovascular and neurological systems to rule out serious conditions.
- Cardiovascular Examination:
- Heart Sounds: The doctor will listen for abnormal heart sounds, murmurs, or signs of heart failure.
- Vital Signs Monitoring: Blood pressure and heart rate will be checked in different positions (lying down, sitting, standing) to detect orthostatic hypotension (a drop in blood pressure when standing).
This step-by-step approach helps identify the cause of syncope and guides the right treatment plan.
- Medical History Review:
Diagnostic Testing
- Once the initial evaluation is complete, your doctor may recommend further diagnostic tests to pinpoint the exact cause of your syncope. These tests are tailored to your symptoms and may include:
- Electrocardiogram (ECG):
- Checks for irregular heart rhythms (arrhythmias) or other heart-related issues.
- Echocardiogram:
- Uses ultrasound to examine the structure and function of your heart, identifying any abnormalities that could cause fainting.
- Holter Monitor:
- A portable device that records your heart’s activity over 24-48 hours to catch intermittent arrhythmias.
- Tilt Table Test:
- Simulates changes in posture (lying down to standing) to diagnose vasovagal syncope by monitoring blood pressure and heart rate responses.
- Neurological Evaluation:
- If a brain-related cause is suspected, imaging tests like CT scans or MRIs may be used to check for issues.
- Blood Tests:
- Screens for conditions like anemia, electrolyte imbalances, or metabolic disorders that could trigger syncope.
- Electrocardiogram (ECG):
San Francisco Syncope Rule
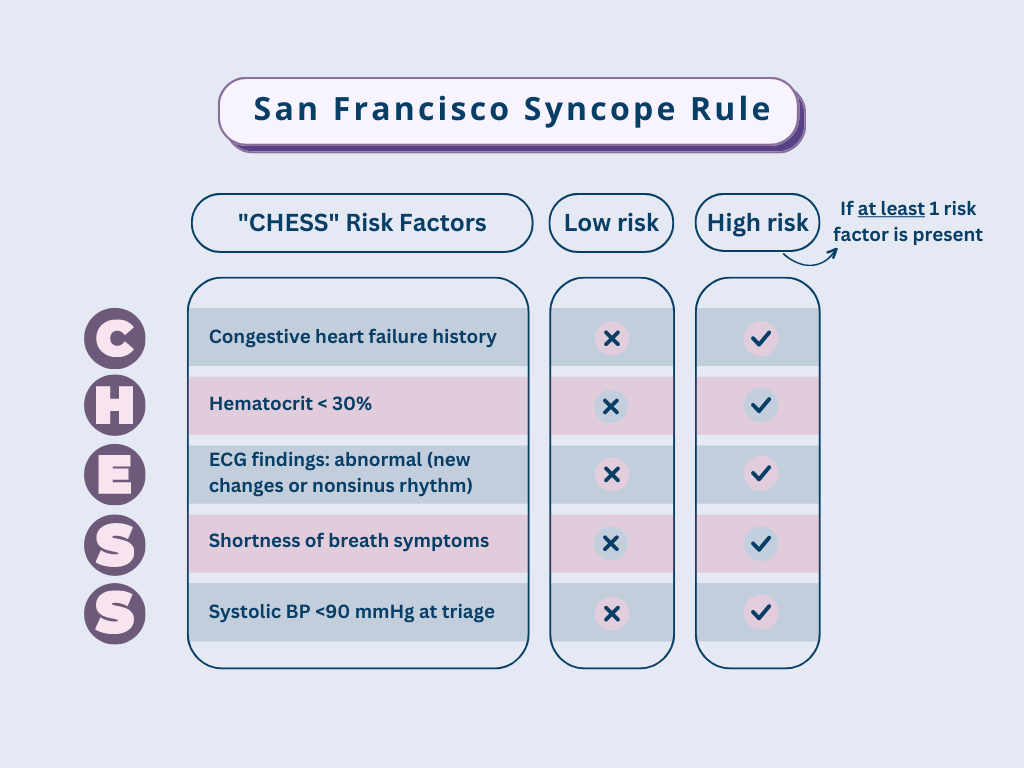
- The San Francisco Syncope Rule (SFSR) is a valuable tool used by healthcare professionals to assess the risk of serious outcomes in patients who experience syncope (fainting). This rule helps identify individuals who may be at high risk for complications, such as death or significant health issues, following a fainting episode.
How Does It Work?
The SFSR evaluates patients based on five key criteria:- History of Heart Failure: Does the patient have a known history of heart failure?
- Abnormal ECG Findings: Are there any irregularities in the electrocardiogram (ECG)?
- Shortness of Breath: Does the patient report difficulty breathing?
- Low Blood Pressure: Is the systolic blood pressure below 90 mmHg?
- Hematocrit Level: Is there evidence of anemia (low red blood cell count)?
Why is it Important?
The SFSR helps doctors:- Prioritize Care: Identify patients who need immediate attention.
- Reduce Risks: Prevent complications by catching serious conditions early.
- Streamline Decisions: Make informed choices about patient management.
Criteria of the San Francisco Syncope Rule:
- The San Francisco Syncope Rule (SFSR) uses the mnemonic CHESS to help healthcare providers quickly identify patients at higher risk of serious outcomes after a syncope episode. Here’s what CHESS stands for and why each criterion matters:
C – History of Congestive Heart Failure
- Why It Matters: Patients with a history of congestive heart failure are at greater risk for cardiovascular complications following syncope.
H – Hematocrit < 30%
- Why It Matters: Low hematocrit levels (indicating anemia) can contribute to fainting and may signal underlying health issues that need attention.
E – Abnormal ECG
- Why It Matters: New or unusual findings on an electrocardiogram (ECG), such as irregular heart rhythms, suggest potential heart problems that could lead to serious outcomes.
S – Shortness of Breath
- Why It Matters: Difficulty breathing (dyspnea) may point to cardiac or respiratory issues, increasing the risk of complications.
S – Triage Systolic Blood Pressure < 90 mmHg
- Why It Matters: Low blood pressure at the time of evaluation indicates hemodynamic instability, which is linked to a higher risk of adverse events.
Implications of the Criteria
- If any one of the CHESS criteria is present in a patient who has experienced syncope, they cannot be classified as “low risk” for serious outcomes. These serious outcomes are defined broadly and include:
- Death
- Myocardial Infarction (heart attack)
- Arrhythmia (abnormal heart rhythms)
- Pulmonary Embolism (blood clot in the lungs)
- Stroke
- Subarachnoid Hemorrhage (bleeding in the brain)
- Significant Hemorrhage (major bleeding)
Why This Matters
The presence of even one CHESS criterion signals that the patient needs immediate attention and further evaluation to prevent potentially life-threatening complications. By identifying high-risk patients early, healthcare providers can take swift action to ensure the best possible outcomes.
Management of Syncope
- Basic management that is recommended for all the patients is:
Position
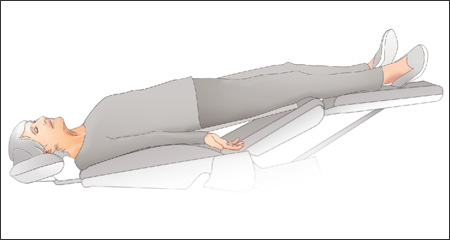
- The first and most critical step in managing syncope is to position the patient correctly. Here’s what to do:
- Place the Patient in a Supine or Anti-Trendelenburg Position:
- Lay the patient flat on their back (supine) or with their head slightly lower than their feet (anti-Trendelenburg).
- Elevate their legs slightly to improve blood flow.
- Why This Helps:
- This position stops the progression of syncope symptoms by increasing blood return to the heart from the extremities.
- It helps restore proper circulation and prevents further episodes of fainting.
- Place the Patient in a Supine or Anti-Trendelenburg Position:
Circulation
- After positioning the patient, the next steps in managing syncope involve a detailed assessment and immediate interventions to stabilize their condition. Here’s what healthcare providers typically do:
- Assessment of Vital Signs:
- Check the patient’s pulse, blood pressure, and signs of shock.
- A rapid heart rate or low blood pressure may indicate poor circulation, which needs urgent attention.
- Intravenous (IV) Access:
- Establishing IV access allows for fluid resuscitation, especially if the patient is hypotensive (low blood pressure) or dehydrated.
- Fluids help restore blood volume and improve circulation.
- Cardiac Monitoring:
- Continuous monitoring of the heart rhythm is essential to detect arrhythmias (irregular heartbeats), which can be a cause or consequence of syncope.
- Pharmacologic Support:
- If the patient has significant hypotension or poor perfusion, medications like vasopressors may be administered to stabilize blood pressure and improve blood flow to vital organs.
- Assessment of Vital Signs:
Airway
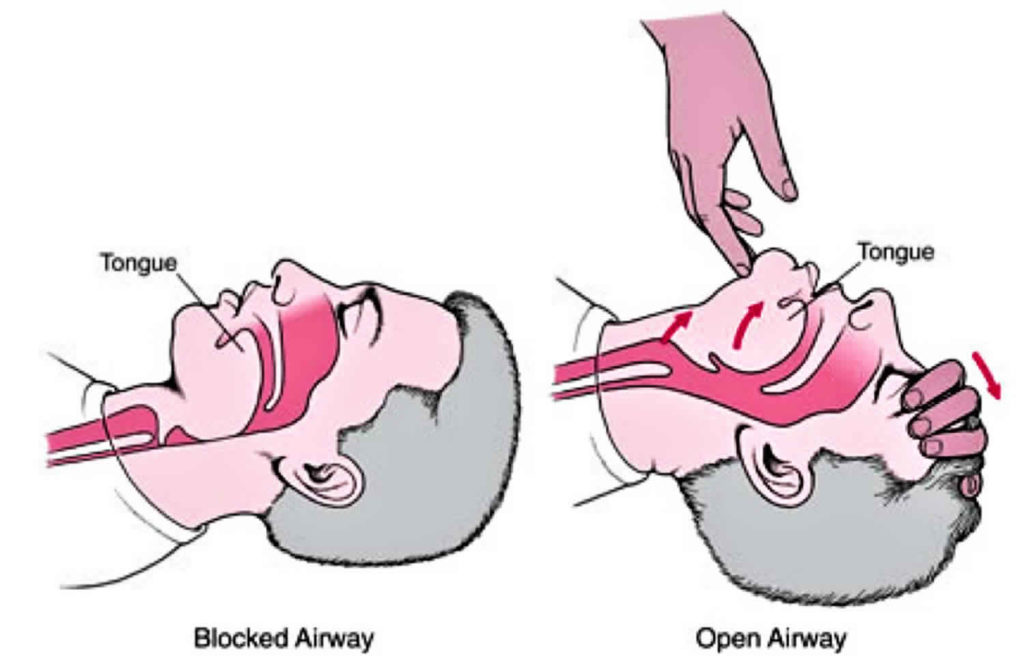
- Maintaining a patent (open) airway is absolutely critical during a syncope episode, especially if the patient loses consciousness. Here’s how healthcare providers ensure the airway stays clear and the patient can breathe properly:1. Positioning
- If the patient is unconscious but breathing, place them in the recovery position (on their side).
- Why It Helps: This position prevents aspiration (inhaling vomit or fluids) and keeps the airway open.
- Provide supplemental oxygen if the patient shows signs of respiratory distress or hypoxia (low oxygen levels).
- Why It Helps: Oxygen ensures the brain and other vital organs receive enough oxygen to function properly.
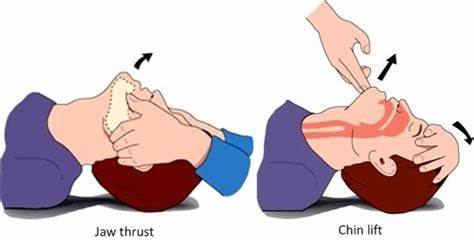
- Basic Airway Adjuncts:
- Use of oral or nasal airways to keep the airway open.
- Supraglottic Airway Devices:
- Devices like laryngeal mask airways (LMAs) that sit above the vocal cords to maintain airflow.
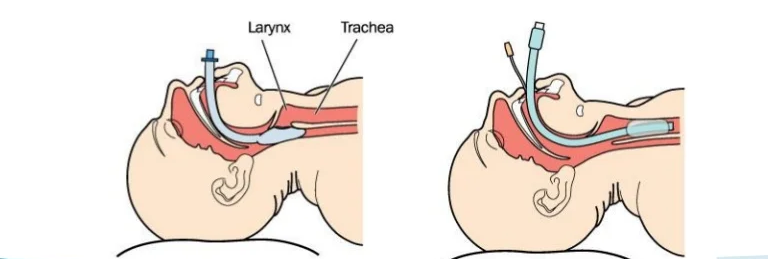
- Endotracheal Intubation:
- Inserting a tube through the mouth or nose into the trachea to secure the airway.
- Surgical Airway:
- In extreme cases, a cricothyrotomy (creating an opening in the throat) may be necessary.
1. Intubation Techniques
i. Orotracheal Intubation
- IndicationsThis procedure is used for patients who:
- Require Mechanical Ventilation: For example, during surgery, severe respiratory failure, or cardiac arrest.
- Are at High Risk for Aspiration: Such as unconscious patients who may inhale vomit or fluids into their lungs.
- Preparation:
- The patient is positioned lying flat with the neck slightly extended.
- The healthcare provider prepares the necessary equipment, including the ETT, laryngoscope, and suction device.
- Direct Laryngoscopy:
- A laryngoscope (a tool with a light and blade) is used to lift the tongue and epiglottis, allowing the provider to visualize the vocal cords.
- Tube Insertion:
- The ETT is gently guided through the vocal cords and into the trachea.
- A small balloon at the end of the tube is inflated to secure it in place and prevent air leakage.
- Confirmation:
- Proper placement is confirmed by listening for breath sounds, checking for chest rise, and using a capnograph (a device that measures carbon dioxide levels).
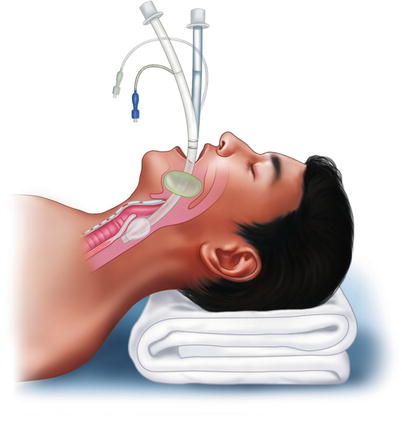
ii. Nasotracheal Intubation
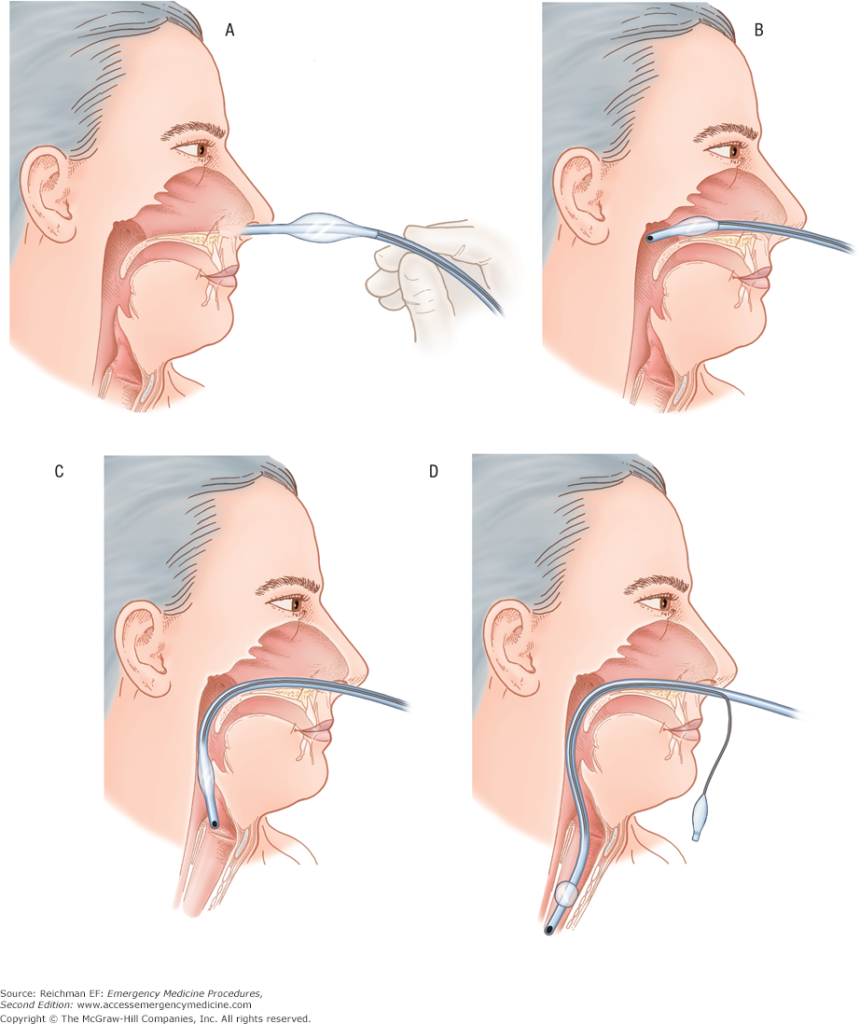
- DefinitionNasotracheal intubation is the insertion of an endotracheal tube (ETT) through the nose and into the trachea (windpipe). This method is often used when oral intubation isn’t feasible or ideal.
IndicationsThis procedure is suitable for:
- Conscious Patients with Intact Gag Reflexes: Patients who are awake or semi-conscious but need intubation.
- Limited Mouth Opening: Patients who cannot open their mouth wide enough for orotracheal intubation, such as those with jaw injuries or trismus (lockjaw).
ConsiderationsNasotracheal intubation is not recommended in cases of:
- Suspected Skull Fractures: Due to the risk of the tube entering the brain cavity.
- Significant Facial Trauma: Nasal injuries or fractures can complicate the procedure.
Procedure
- Preparation:
- The patient is positioned comfortably, often with the head slightly extended.
- The nasal passage is prepared with a vasoconstrictor to reduce bleeding and lubricant to ease tube insertion.
- Tube Insertion:
- The ETT is gently advanced through the nostril and guided into the trachea.
- A laryngoscope may be used to visualize the vocal cords and assist in guiding the tube.
- Confirmation:
- Proper placement is confirmed by listening for breath sounds, checking for chest rise, and using a capnograph (a device that measures carbon dioxide levels).
iii. Laryngeal Mask Airway (LMA)

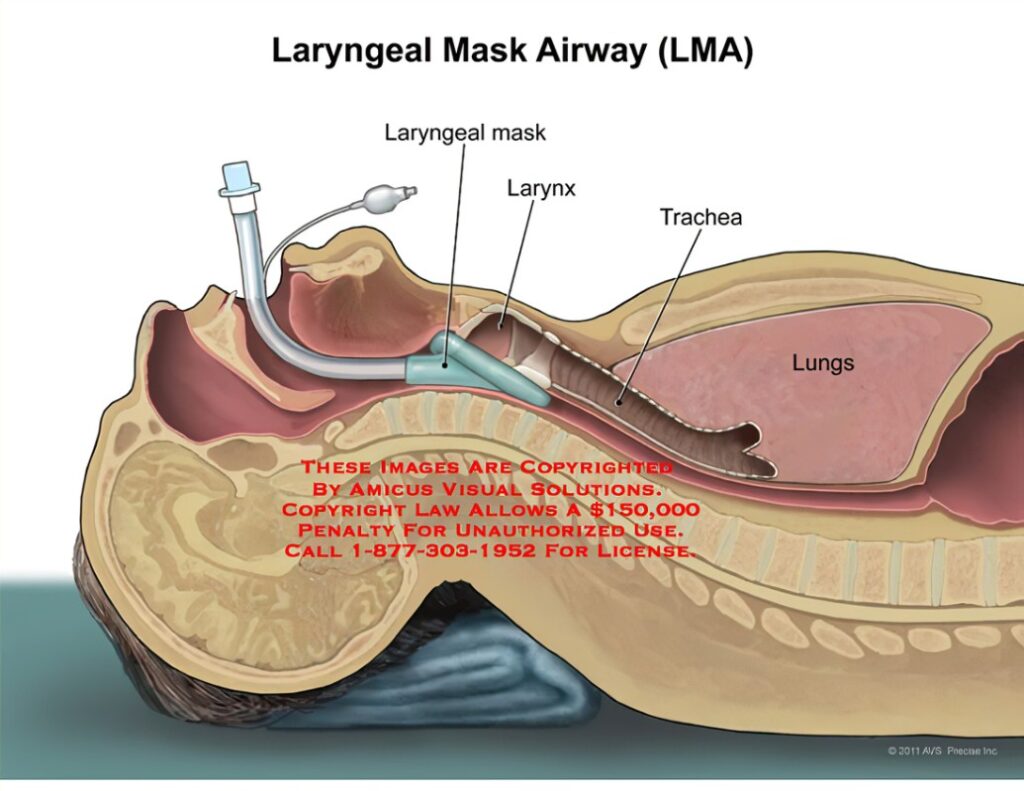
- DefinitionThe LMA is a supraglottic airway device that sits above the vocal cords, creating a seal around the larynx. It allows for ventilation without the need for inserting a tube into the trachea.IndicationsThe LMA is particularly useful in situations where:
- Intubation is Difficult: For example, in patients with challenging anatomy or limited mouth opening.
- Rapid Airway Control is Needed: Such as in emergencies or during short surgical procedures.
- Full Anesthesia is Not Required: It can be used in conscious or lightly sedated patients.
- Classic LMA:
- The most common type, used for routine airway management.
- Ideal for short procedures or as a backup during difficult intubations.
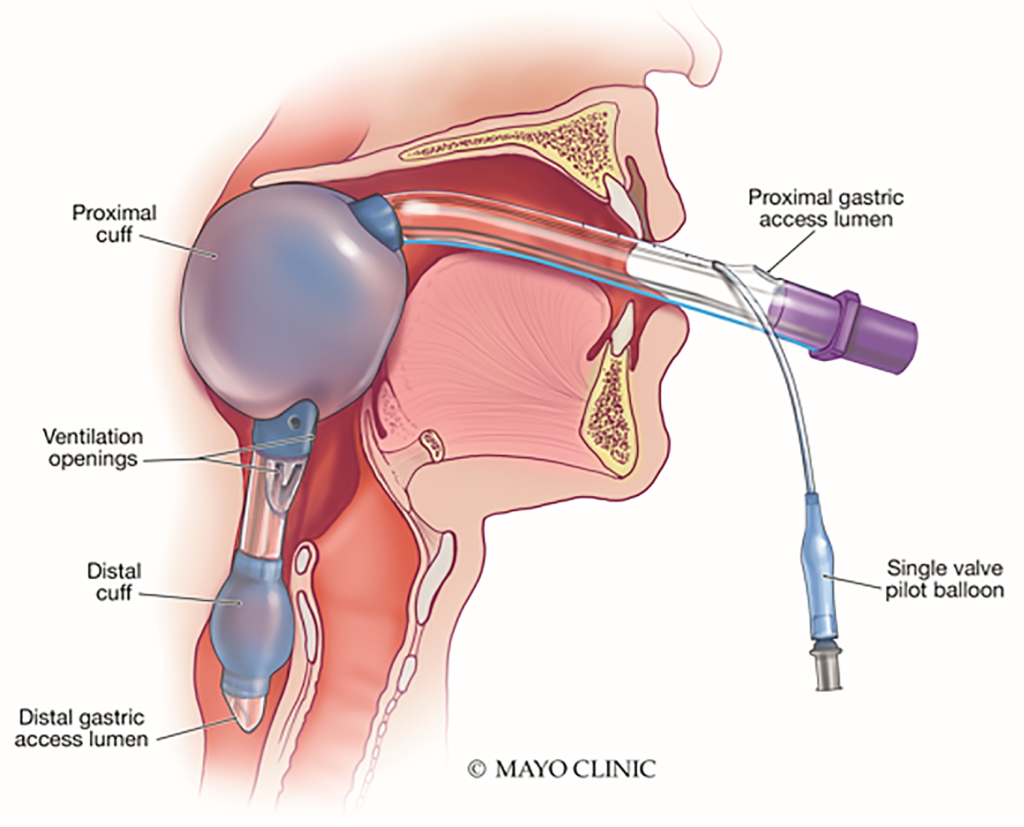
- ProSeal LMA:
- Designed with a gastric drainage tube to reduce the risk of aspiration.
- Often used in longer procedures or when higher airway pressures are needed.
- Preparation:
- The patient is positioned correctly, and the LMA is lubricated for easy insertion.
- Insertion:
- The LMA is gently inserted through the mouth and advanced until it sits above the larynx.
- A cuff is inflated to create a seal, ensuring proper ventilation.
- Confirmation:
- Proper placement is confirmed by listening for breath sounds, checking for chest rise, and using a capnograph (a device that measures carbon dioxide levels).
iv. Blind Insertion Devices
- Blind Insertion Devices are lifesaving tools used in emergencies when traditional intubation methods fail or aren’t feasible. Here’s a clear and concise explanation of what they are and how they work:Examples
- Combitube:
- A double-lumen tube that can be inserted blindly into the esophagus or trachea.
- Allows ventilation regardless of placement.
- King LT:
- A single-lumen tube designed to sit in the esophagus, with ventilation ports aligning with the larynx.
- Traditional Intubation Fails: For example, due to difficult anatomy or lack of equipment.
- Direct Visualization of the Glottis is Not Possible: Such as in pre-hospital settings or during CPR.
- Rapid Airway Control is Needed: When time is critical, and immediate ventilation is required.
- Preparation:
- The patient is positioned correctly, and the device is lubricated for easy insertion.
- Insertion:
- The device is inserted blindly through the mouth and advanced until resistance is felt.
- A cuff is inflated to create a seal, ensuring proper ventilation.
- Confirmation:
- Proper placement is confirmed by listening for breath sounds, checking for chest rise, and using a capnograph (a device that measures carbon dioxide levels).
- Combitube:
2. Surgical Airways
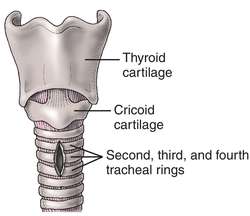
i. Cricothyrotomy
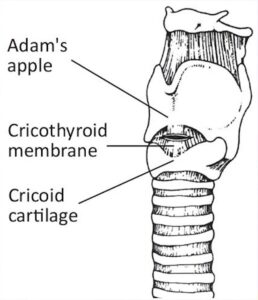
- DefinitionCricothyrotomy is an emergency surgical procedure that involves making an incision through the cricothyroid membrane (a thin tissue between the thyroid and cricoid cartilage) to create an airway.IndicationsThis procedure is used in life-threatening situations where:
- Other Airway Methods Fail: For example, when intubation is impossible due to severe swelling, trauma, or obstruction.
- Severe Airway Obstruction: Such as in cases of facial trauma, burns, or foreign body obstruction.
- Time is Critical: When immediate airway access is needed to save a patient’s life.
- Quicker to Perform: Compared to a tracheotomy, it’s faster and simpler, making it ideal for emergencies.
- Fewer Complications: It avoids major blood vessels and nerves, reducing the risk of bleeding or nerve damage.
- Life-Saving: Provides immediate airway access when other methods are not feasible.
- Preparation:
- The patient is positioned with the neck extended to expose the cricothyroid membrane.
- The area is cleaned and sterilized.
- Incision:
- A horizontal incision is made through the skin and cricothyroid membrane.
- A tube or airway device is inserted to maintain the opening.
- Confirmation:
- Proper placement is confirmed by listening for breath sounds and checking for chest rise.
ii. Tracheotomy
- DefinitionA tracheotomy is a surgical procedure that involves making an incision in the neck and creating an opening directly into the trachea (windpipe). A tube is then inserted to maintain the airway.IndicationsThis procedure is typically performed for:
- Long-Term Ventilation Needs: For patients who require mechanical ventilation for an extended period.
- Prolonged Airway Access: Such as in cases of severe airway obstruction, trauma, or neurological conditions that impair breathing.
- Chronic Conditions: For patients with conditions like ALS, spinal cord injuries, or severe sleep apnea.
- Complexity: Tracheotomy is more complex than cricothyrotomy and is usually performed in a controlled setting, such as an operating room.
- Long-Term Care: Requires regular cleaning and monitoring to prevent infections or complications.
- Risks: Potential risks include bleeding, infection, and damage to surrounding structures.
- Preparation:
- The patient is positioned with the neck extended, and the area is cleaned and sterilized.
- Incision:
- A horizontal or vertical incision is made in the lower neck to access the trachea.
- A small opening is created in the trachea, and a tracheostomy tube is inserted.
- Confirmation:
- Proper placement is confirmed by listening for breath sounds and checking for chest rise.
Breathing
- Breathing is a critical aspect of syncope management, and ensuring the patient is breathing effectively is a top priority. Here’s a clear and concise guide to assessing and supporting breathing during a syncope episode:1. Respiratory Assessment
- Monitor Respiratory Rate and Effort:
- Check how fast and deeply the patient is breathing.
- Look for signs of respiratory distress, such as labored breathing, use of accessory muscles, or flaring nostrils.
- Listen for Abnormal Breath Sounds:
- Wheezing, gurgling, or stridor (high-pitched sounds) may indicate an airway obstruction or other issues.
- If the patient shows inadequate breathing (e.g., shallow breaths, irregular breathing, or apnea), bag-mask ventilation may be needed.
- How It Works: A mask is placed over the patient’s nose and mouth, and a bag is squeezed to deliver oxygen-rich air into the lungs.
- Why It’s Important: This provides immediate support until the patient regains spontaneous breathing or advanced care is available.
- Use pulse oximetry to track the patient’s oxygen saturation levels (SpO2).
- Normal SpO2 levels are 95-100%.
- If levels drop below 90%, it indicates hypoxia (low oxygen), and immediate action is needed.
- Why It’s Important: Continuous monitoring ensures the patient maintains adequate oxygenation, preventing complications like brain damage or organ failure.
- Monitor Respiratory Rate and Effort:
Definitive care
- Definitive Care for syncope focuses on stabilizing the patient, addressing the underlying cause, and preventing further episodes. Here’s a clear and concise guide to providing effective care during and after a syncope episode:1. Administration of Oxygen
- When to Use: Oxygen can be administered during or after a syncope episode if the patient shows signs of hypoxia (low oxygen levels) or respiratory distress.
- Why It’s Important: Oxygen helps restore normal oxygen levels, supporting brain function and overall recovery.
- What to Monitor:
- Blood Pressure: Check for hypotension (low blood pressure) or orthostatic changes.
- Heart Rate: Look for bradycardia (slow heart rate) or tachycardia (fast heart rate).
- Respiratory Rate: Ensure the patient is breathing adequately.
- Why It’s Important: Continuous monitoring helps detect abnormalities early and guides treatment decisions.
- Aromatic Ammonia:
- A small ampule can be crushed and held near the patient’s nose to stimulate breathing and improve alertness.
- Why It’s Important: This can help revive the patient quickly by stimulating the respiratory and nervous systems.
- What to Do: Remove or loosen tight clothing like ties, belts, collars, or restrictive garments.
- Why It’s Important: Tight clothing can restrict blood flow and breathing, worsening the episode. Loosening it helps improve circulation and comfort.
Drugs Used in Treatment of Syncope
- Syncope (fainting) can sometimes require medication to prevent episodes and reduce complications. Here’s a clear and concise overview of the commonly used drugs and how they help:
1. Fludrocortisone- How It Works: Helps increase blood volume and improve blood pressure, especially in cases of orthostatic hypotension (low blood pressure when standing up).
- Why It’s Used: Prevents fainting by stabilizing blood pressure.
- How It Works: An alpha-agonist that constricts blood vessels, raising blood pressure.
- Why It’s Used: Effective for patients with orthostatic hypotension or neurogenic syncope.
- How It Works: Stimulates the nervous system to increase heart rate and blood pressure.
- Why It’s Used: Can treat vasodepressor carotid sinus syndrome, but its use is limited due to potential side effects like anxiety or high blood pressure.
- How It Works: Constricts blood vessels to improve blood flow and prevent fainting.
- Why It’s Used: Effective for vasodepressor carotid sinus syndrome, but long-term use is limited due to side effects like nausea or headaches.
- How It Works: These antidepressants may help regulate the nervous system and prevent vasovagal syncope (fainting due to a sudden drop in heart rate and blood pressure).
- Why It’s Used: Promising for managing vasovagal syncope, but more research is needed to confirm their effectiveness.
Dental Considerations
- Syncope (fainting) is one of the most common medical emergencies in dental offices, accounting for about 50% of all emergencies reported by dentists. Here’s what you need to know to handle syncope effectively in a dental setting:Why Syncope Happens in Dental Offices
- Anxiety and Stress:
- Many patients experience dental anxiety, which can trigger a vasovagal response, leading to fainting.
- Pain or Fear:
- The sight of needles, blood, or dental instruments can cause a sudden drop in heart rate and blood pressure.
- Prolonged Sitting:
- Sitting in the dental chair for extended periods, especially in a reclined position, can lead to orthostatic hypotension (a drop in blood pressure when standing up).
- Young Adults: Often due to anxiety or stress.
- Patients with a History of Syncope: Those who have fainted before are more likely to experience it again.
- Anxious Patients: Individuals with dental phobia or high stress levels.
- Pre-Treatment Assessment:
- Ask about a history of fainting, anxiety, or medical conditions that could increase the risk.
- Manage Anxiety:
- Use calming techniques, such as explaining procedures clearly or offering sedation options.
- Positioning:
- Keep the patient in a semi-reclined position rather than fully reclined to improve blood flow.
- Monitor Vital Signs:
- Check blood pressure and heart rate before and during treatment, especially for high-risk patients.
- Position the Patient:
- Lay the patient flat on their back with their legs slightly elevated to improve blood flow to the brain.
- Ensure an Open Airway:
- Check breathing and provide oxygen if needed.
- Monitor Vital Signs:
- Keep track of blood pressure, heart rate, and oxygen levels.
- Stay Calm and Reassure the Patient:
- Most patients recover quickly with proper care.
- Anxiety and Stress:
Risk Factors for Syncope in Dental Settings
Syncope (fainting) during dental procedures can be triggered by a variety of factors. Understanding these risks helps dental professionals prevent and manage syncope effectively. Here’s a breakdown of the key risk factors:
1. Psychogenic FactorsAnxiety and Fear: Many patients experience dental anxiety or fear of needles, pain, or the dental environment, which can trigger a vasovagal response.
Emotional Stress: Stressful situations, such as recalling past negative dental experiences, can increase the risk of fainting.
High-Risk Patients: Those with a history of dental phobia or anxiety are more prone to syncope.
Prolonged sitting or standing:
Sitting upright in the dental chair for too long can cause blood to pool in the legs, reducing blood flow to the brain.
Standing suddenly after a procedure can lead to orthostatic hypotension (a sudden drop in blood pressure).
Dehydration: Not drinking enough water before an appointment can lower blood volume and increase the risk of fainting.
Hunger or Exhaustion: Skipping meals or being overly tired can contribute to low blood sugar and reduced energy levels.
Hot Environments: A warm or stuffy dental office can cause vasodilation (widening of blood vessels), leading to a drop in blood pressure.
Cardiovascular Issues: Conditions like arrhythmias, heart disease, or low blood pressure can predispose patients to syncope.
Previous Episodes: Patients who have fainted before, especially in medical or dental settings, are at higher risk.
Medications: Certain medications, such as blood pressure drugs or sedatives, can increase the likelihood of fainting.
Signs and Symptoms of Syncope
- Syncope (fainting) often comes with warning signs that can be divided into early and late stages. Recognizing these symptoms helps dental professionals act quickly to prevent a full episode. Here’s what to look for:
Early SignsThese are the first warning signals that a patient may be about to faint:
- Feelings of Warmth: The patient may suddenly feel hot or flushed.
- Pallor: The skin may turn pale or ashen-grey.
- Excessive Sweating (Diaphoresis): Cold, clammy sweat is a common early sign.
- Nausea: The patient may feel queasy or sick to their stomach.
- Slight Hypotension: A mild drop in blood pressure may occur.
- Tachycardia: The heart rate may increase temporarily.
Late SignsIf early signs are missed or ignored, these more severe symptoms may follow:
- Pupillary Dilation: The pupils may widen.
- Yawning: Frequent yawning can signal reduced oxygen levels.
- Cold Extremities: The hands and feet may feel cold to the touch.
- Significant Hypotension: A sharp drop in blood pressure occurs.
- Bradycardia: The heart rate may slow down dramatically.
- Visual Disturbances: Blurred vision, tunnel vision, or blackouts may occur.
- Dizziness: The patient may feel lightheaded or unsteady.
- Loss of Consciousness: If untreated, the patient may faint.
Emergency Management Protocols for Syncope in Dental Settings
Syncope (fainting) is a common medical emergency in dental offices, and knowing how to respond quickly and effectively is crucial. Here’s a step-by-step guide to managing syncope during a dental procedure:
1. Discontinue Treatment
- What to Do: Immediately stop any ongoing dental procedures.
- Why It’s Important: This ensures the patient’s safety and allows you to focus on their immediate needs.
2. Positioning
- What to Do: Place the patient in a supine position (flat on their back) with their legs slightly elevated (Trendelenburg position).
- Why It’s Important: This position promotes venous return, improving blood flow to the brain and helping the patient recover faster.
3. Assess Vital Signs
- What to Do:
- Check the patient’s airway to ensure it’s clear.
- Monitor pulse and blood pressure to assess circulation.
- Why It’s Important: Identifying abnormalities helps guide further treatment.
4. Oxygen Administration
- What to Do: Provide supplemental oxygen via a mask or nasal cannula.
- Why It’s Important: Oxygen enhances cerebral perfusion, ensuring the brain gets enough oxygen to function properly.
5. Stimulation Techniques
- What to Do: Use aromatic ammonia inhalants (crushed ampules) to stimulate consciousness through irritant fumes.
- Why It’s Important: This can help revive the patient quickly by stimulating the respiratory and nervous systems.
6. Post-Syncopal Care
- If recovery occurs within 15 minutes:
- Postpone further dental treatment for the day.
- Monitor the patient until they are stable and able to sit up without symptoms.
- If No Recovery After 15 Minutes or Vital Signs Deteriorate:
- Activate Emergency Medical Services (EMS) immediately.
- Continue monitoring and providing supportive care until help arrives.
Preventive Measures for Syncope in Dental Settings
- Preventing syncope (fainting) during dental visits is essential for ensuring patient safety and comfort. Here are some practical steps dental professionals can take to minimize the risk:
1. Conduct Thorough Medical Histories
- What to Do: Ask about a patient’s medical history, including any history of fainting, anxiety, or cardiovascular issues.
- Why It’s Important: Identifying at-risk patients allows you to tailor care and take extra precautions.
2. Advise Patients to Eat Lightly Before Appointments
- What to Do: Encourage anxious patients to have a light meal or snack before their visit.
- Why It’s Important: This helps maintain stable blood glucose levels and prevents fainting due to low blood sugar.
3. Use Anxiety Management Techniques
- What to Do: Offer nitrous oxide sedation (laughing gas) or other calming methods for anxious patients.
- Why It’s Important: Reducing anxiety lowers the risk of a vasovagal response, which can trigger syncope.
4. Treat Patients in a Reclined Position
- What to Do: Position patients in a semi-reclined or reclined position during treatment.
- Why It’s Important: This improves blood flow to the brain and reduces the risk of orthostatic hypotension (a sudden drop in blood pressure when standing up).
CONCLUSION
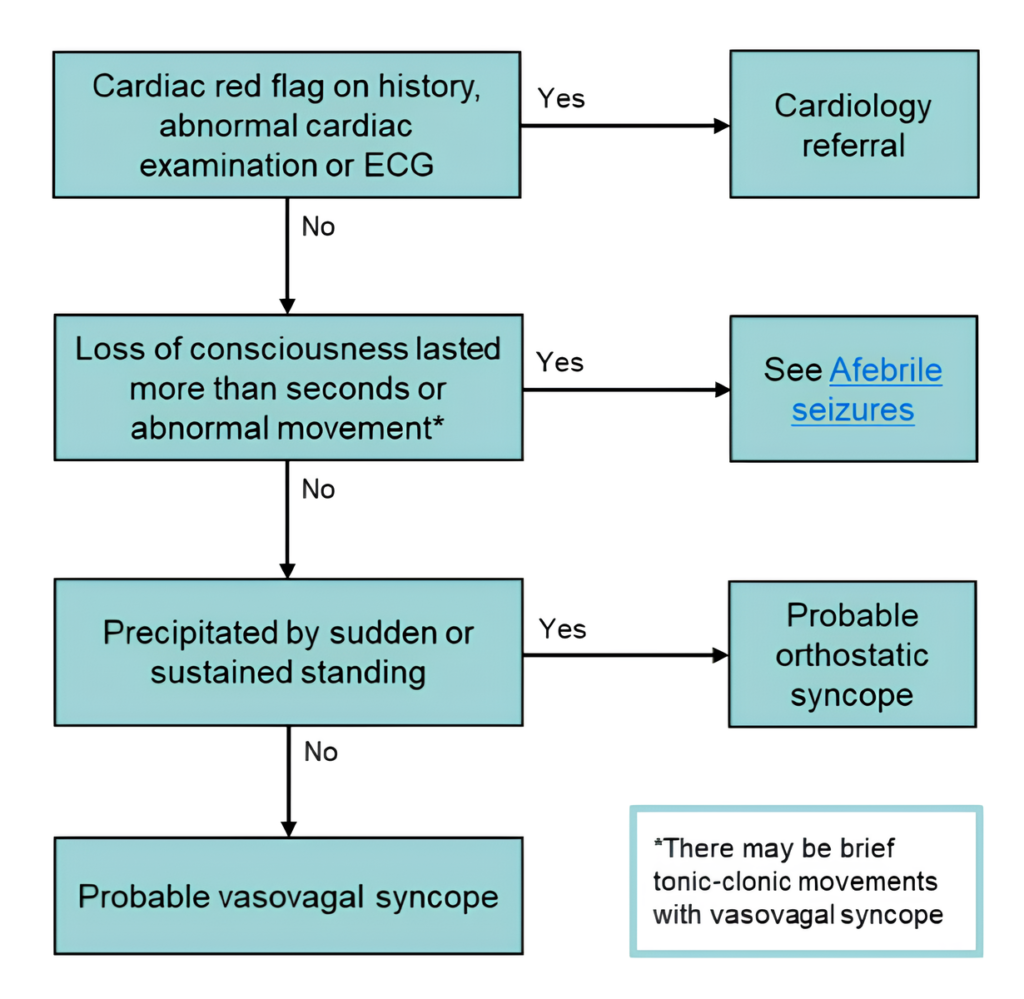
- Syncope, a transient loss of consciousness due to a temporary drop in blood flow to the brain, is a complex condition with a wide range of causes. It can stem from reflex (neurally mediated), orthostatic, or cardiac origins. While many cases are benign and linked to situational or vasovagal triggers, some may signal serious underlying conditions that could lead to significant health risks.Key Points to Remember
- Evaluation:
- Start with a detailed history and physical exam, focusing on the event’s circumstances, associated symptoms, and risk factors.
- Use diagnostic tools like ECG, imaging, or prolonged monitoring to identify the root cause.
- Management:
- For benign cases, patient education and lifestyle changes (e.g., staying hydrated, avoiding triggers) are often sufficient.
- For cardiac-related syncope, more intensive interventions like medications or device therapy (e.g., pacemakers) may be necessary.
- Clinical Vigilance:
- Differentiating between benign episodes and those requiring urgent care is critical.
- Early identification of serious causes can prevent complications and improve outcomes.
- Evaluation:



