Previously, it was known as CYSTIC APICAL PERIODONTITIS. The radicular cyst is the most common odontogenic cyst. It occurs as a result of bacterial infection and pulpal necrosis which leads to inflammatory stimulation of the epithelial cell rests of Malassez along the periodontal ligament area of the tooth. Most cases of the radicular cyst are asymptomatic and they are diagnosed accidentally during routine radiographic examination.Radicular cyst is also known as periapical radicular cyst, radicular cyst dental, periapical cyst, root end cyst, and dental radicular cyst.
What is a cyst?
A cyst is a closed cavity or sac internally lined with epithelium, the center of which is filled with fluid or semisolid material.
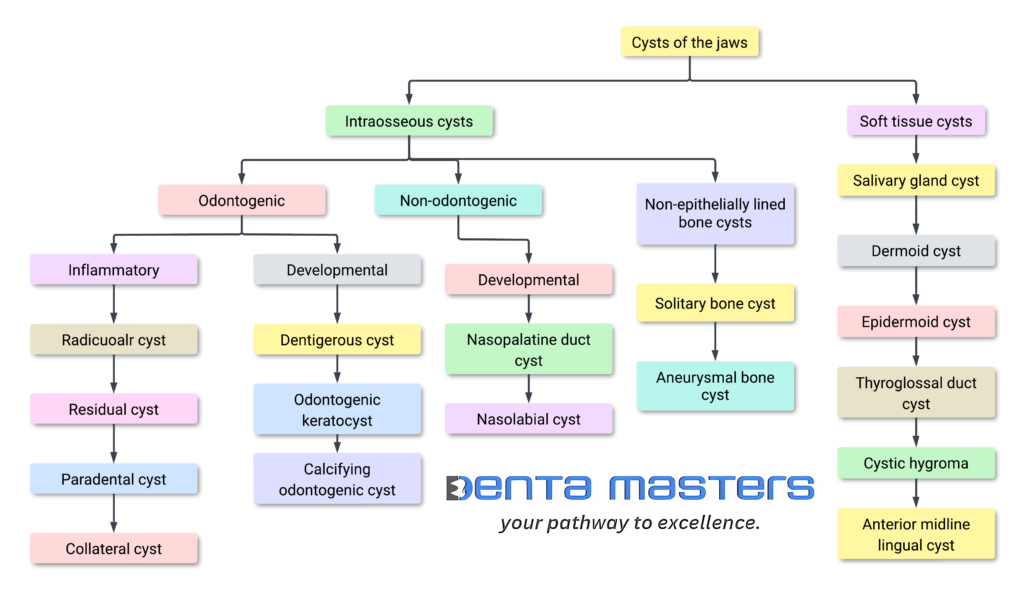
Classification of Cyst
Epidemiology
Most common odontogenic cyst (52% of jaw cystic lesions)
Most common in 4th & 5th decades but occurs over wide age range.
Periapical cysts result from infection of the tooth, which spreads to the apex and into the adjacent bone. This leads to apical periodontitis, granuloma formation, and eventual cyst formation. These cysts are therefore centred on the apex of the tooth and tend to be small, usually <1 cm.
Physical, chemical, or bacterial injury causing pulpal death results in stimulation of the epithelial rests of Malassez present in the periodontal ligament.
Radicular cysts are formed by the resorption of the periapical portions of alveolar bone by immune-inflammatory mechanisms.
These mechanisms include activities carried out by cells that are pivotal in bone formation and resorption, such as osteoblasts, osteocytes, and osteoclasts.
The formation of radicular cysts is due to the release of inflammatory cytokines and growth factors.
Two hypotheses are proposed for the growth of the cyst:
Nutritional deficiency theory:
It proposes that periradicular inflammatory changes cause the epithelium to proliferate.
Epithelium grows into mass of cells
The centre loses nutrition from peripheral tissues.
Necrosis is in the centre.
cavity lined by stratified squamous epithelium
Cyst formed
Abscess theory:
It proposes that an abscess cavity is formed in the connective tissue and is then surrounded with proliferating epithelial tissue, thereby producing a cyst.
Types of Radicular cyst
(described by Nair)
Periapical pocket cyst:
The cyst contains an epithelial-lined cavity that is open towards the root canal of the affected tooth.
originally designated as bay cyst and is now redesignated as the periapical pocket cyst.
initiated by accumulation of neutrophils around the apical foramen in response to microbial biofilm present in the apical portion of the root canal.
This forms a micro-abscess. The apical pouch seals the infected root canals with the micro-abscess from the periapical tissue.
Periapical true cyst: characterised by cavities that are completely enclosed in epithelial lining and are totally independent of the root canal of the affected tooth
Symtoms
Asymptomatic: In many cases, Radicular cyst may not cause any symptoms and may only be discovered incidentally during routine dental X-rays.
Dull, Persistent Discomfort: Some individuals may experience mild, dull discomfort or a feeling of pressure in the affected tooth region.
Swelling: Swelling of the gums or soft tissues around the affected tooth may occur, especially if the cyst becomes infected or enlarges.
Abscess Formation: In more severe cases, the cyst may become secondarily infected, leading to the formation of an abscess and associated symptoms such as pain, swelling, and pus drainage.
Diagnosis
Negative reaction to electrical or thermal stimuli or other clinical tests.
patient may report history of pain.
Radiographic examination
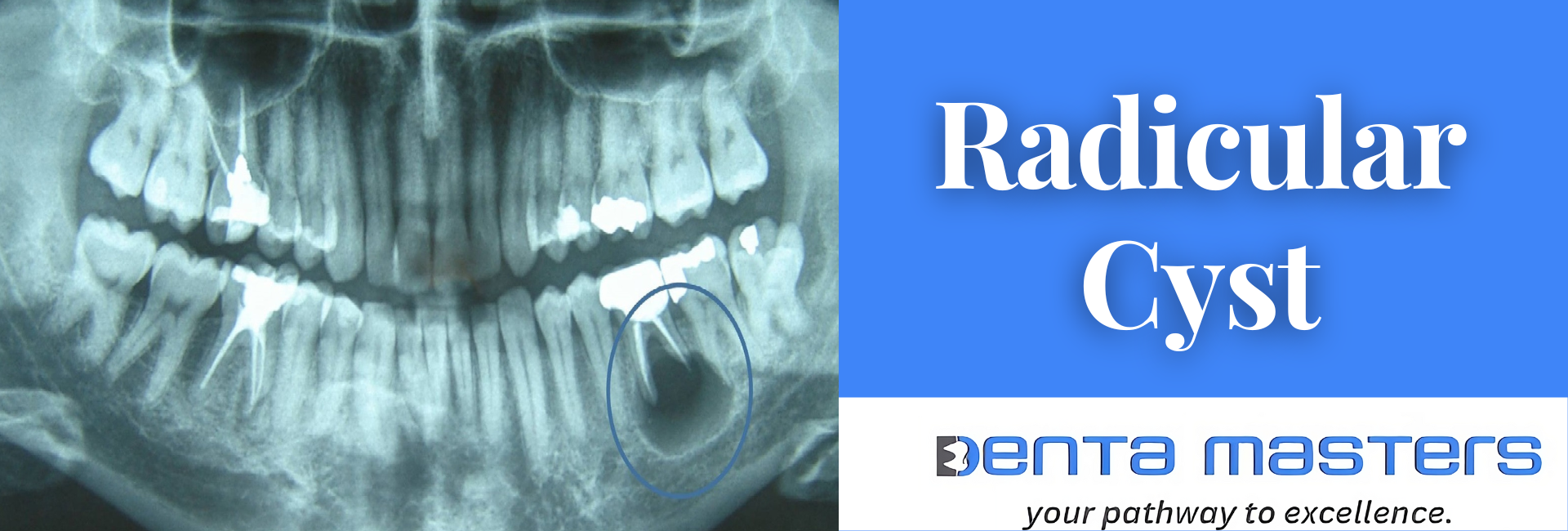
Round to oval radiolucency, often with well-defined cortical border (this border can be lost when infected)
The radiolucent area may be larger than a chronic apical abscess and may include more than one tooth.
Can displace or reabsorb roots of adjacent teeth if they are large.
Neither the size nor the shape of the rarefied area is a definite indication of a cyst.
radiographic examination alone is not sufficient for a diagnosis.
Location
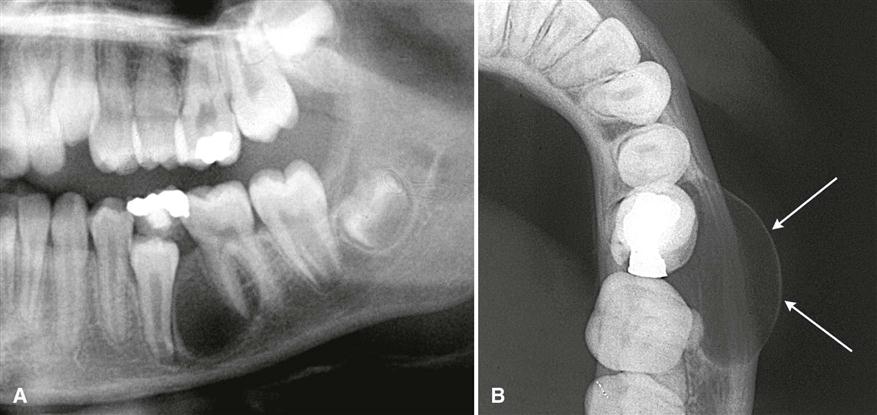
( A) Note the epicenter is apical to the lateral incisor and the presence of a peripheral cortex (arrows). (B) Note the lack of a well-defined peripheral cortex because this cyst was secondarily infected. Also note the root canal of the lateral incisor is abnormally wide and it is visible at the root apex.
Periphery and shape.
The periphery usually has a well-defined cortical border (A). If the cyst becomes secondarily infected, the inflammatory reaction of the surrounding bone may result in loss of this cortex ( B) or alteration of the cortex into a more sclerotic border. The outline of a radicular cyst usually is curved or circular, unless it is influenced by surrounding structures such as cortical boundaries.
(A) Periapical film of a radicular cyst reveals a lesion with a well-defined cortical boundary (arrows). The presence of the inferior cortex of the mandible has influenced the circular shape of the cyst. (B) Coronal cone-beam CT image of a radicular cyst related to the buccal root of a maxillary molar. Note the circular shape of the cyst as it invaginates the maxillary sinus. (Courtesy Dr. Bernard Friedland, Harvard University.)
Effects on Surrounding Structures.
A and B, Two images of a radicular cyst originating from a nonvital deciduous second molar show expansion of the buccal cortical plate to a circular or hydraulic shape (arrows in B) and displacement of the adjacent permanent teeth.
Differential diagnosis
Apical periodontitis is smaller than cystic apical periodontitis.
globulomaxillary cysts
fissural cyst that develops in the upper jaw between the roots of lateral and cuspid teeth.
not the result of death of the pulp and may be marsupialized and later enucleated without involving the vitality of the adjacent teeth.
lateral periodontal cysts, identified by associated periodontal signs and symptoms
incisive canal cysts
aneurysmal bone cysts
traumatic bone cysts, hemorrhagic cysts, or extravasation cysts are hollow cavity lined not by epithelium but by fibrous connective tissue.
fibrous dysplasia
normal bone cavity appears dissociated from the root apex on radiographs taken at different angles, whereas a cyst remains attached to the root apex regardless of the angle at which the radiograph is taken.
Dentigerous cyst: lesion around the crown of an unerupted/impacted tooth.
Keratocystic odontogenic tumour
Lateral radicular cyst: considered a variant of a true peri-apical cyst.
Residual cyst
Bacteriology
A cyst may or may not be infected.
Actinomyces organisms have been isolated from a periapical cyst.
Histopathology
Cavity lined with stratified squamous epithelium derived from epithelial cell rests of Malassez present in the periodontal ligament.
Immunologically competent cells present in the epithelial lining
Immunoglobulins present in the cyst fluid.
The epithelial cell rests of Malassez can become recognized as antigen and may produce an immunologic reaction, which in turn causes lysis of the cystic wall.
the lesion is an asymptomatic apical periodontitis with a cavity lined with stratified squamous epithelium.
Surrounded by connective tissue that is infiltrated by lymphocytes, plasma cells, and polymorphonuclear neutrophils.
Cholesterol clefts, macrophages, and giant cells also present in CT.
Cystic cavity contains debris and eosinophilic material.
Treatment
Treatment of choice – ROOT CANAL THERAPY followed by periodic observation.
Surgery required when lesion fails to resolve or symptoms develop.
Extraction in case of severe bone loss.
Prognosis
Depends on the particular tooth, extent of bone loss and accessibility for treatment.