During pregnancy, women may need to take medications to treat new or existing health conditions. Also, certain vitamins are recommended during pregnancy. Before taking any medication (including over-the-counter medications) or dietary supplement (including medicinal herbs), a pregnant woman should consult a doctor. Women currently taking medications and planning to become pregnant should consult a doctor before pregnancy, if possible, to see if those medications need to be stopped or changed. (See also the Centers for Disease Control and Prevention: Medicine and Pregnancy.)
Medications or other substances taken by a pregnant woman may reach the fetus by crossing the placenta, the same route taken by oxygen and nutrients, which are needed for the fetus’s growth and development. However, those that do not cross the placenta may still harm the fetus by affecting the uterus or the placenta.
Medications or other substances that a pregnant woman takes during pregnancy can affect the fetus in several ways:
No impact on the fetus and its development
Act directly on the fetus, causing damage, abnormal development (leading to birth defects), or death
Alter the function of the placenta, usually by causing blood vessels to narrow (constrict) and thus reducing the supply of oxygen and nutrients to the fetus from the mother (sometimes resulting in the baby being underweight and underdeveloped)
Cause the muscles of the uterus to contract forcefully, indirectly injuring the fetus by reducing its blood supply or triggering preterm labor and delivery
Affect the fetus indirectly (for example, medications that lower the mother’s blood pressure may reduce blood flow to the placenta and thus reduce the supply of oxygen and nutrients to the fetus)
Some medications stay in the body and can have effects after they are stopped. For example, isotretinoin, a medication used to treat skin disorders, is stored in fat beneath the skin and is released slowly over weeks. Isotretinoin can cause birth defects if a woman becomes pregnant within 2 weeks after the medication is stopped. Therefore, women are advised to wait at least 3 to 4 weeks after the medication is stopped before they become pregnant.
How medicine transfer from mother to fetus
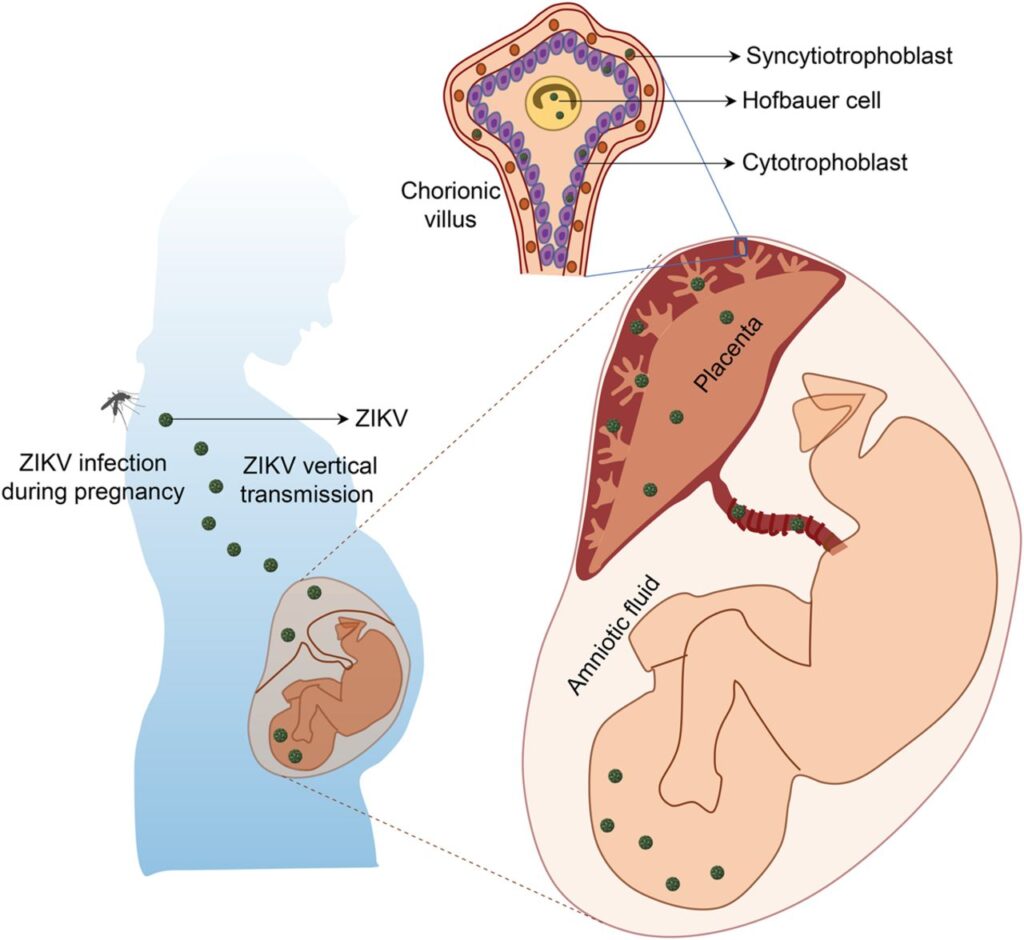
Drugs diffuse across the placenta similarly to the way they cross other epithelial barriers (see Absorption). Whether and how quickly a drug crosses the placenta depends on the drug’s molecular weight, extent of its binding to another substance (e.g., carrier protein), area available for exchange across the placental villi, and amount of drug metabolised by the placenta. Most drugs with a molecular weight of < 500 daltons readily cross the placenta and enter the foetal circulation. Substances with a high molecular weight (e.g., protein-bound drugs) usually do not cross the placenta. One exception is immune globulin G, which may be used to treat disorders such as foetal alloimmune thrombocytopenia or foetal hemachromatosis. Generally, equilibration between maternal blood and foetal tissues takes at least 30 to 60 minutes; however, some drugs do not reach similar concentrations in the maternal and foetal circulation.
Pregnancy and Teratogens
A teratogen is anything a person is exposed to or ingests during pregnancy that’s known to cause foetal abnormalities. Drugs, medicine, chemicals, certain infections, and toxic substances are examples of teratogens.
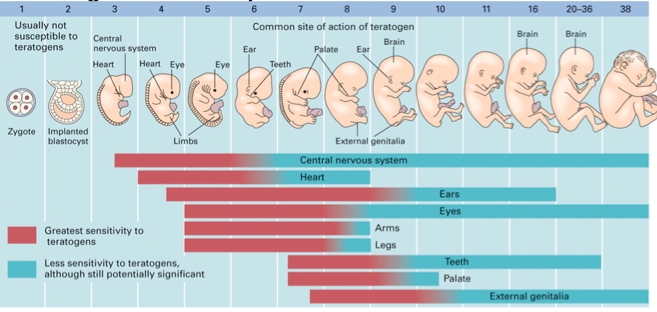
Before the 20th day after fertilization: Drugs given at this time typically have an all-or-nothing effect, killing the embryo or not affecting it at all. Teratogenesis is unlikely during this stage.
During organogenesis (between 20 and 56 days after fertilization): Teratogenesis is most likely at this stage. Drugs that enter the embryo during this stage may cause spontaneous abortion, a sublethal gross anatomical defect (a true teratogenic effect), covert embryopathy (a permanent subtle metabolic or functional defect that may manifest later in life), or an increased risk of childhood cancer (for example, when the mother is given radioactive iodine to treat thyroid cancer); or the drugs may have no discernible effect.
After organogenesis (in the second and third trimesters): Teratogenesis is unlikely, but drugs may alter the growth and function of normally formed fetal organs and tissues. As placental metabolism increases, doses must be higher for adverse fetal effects to occur.
list of Teratogens
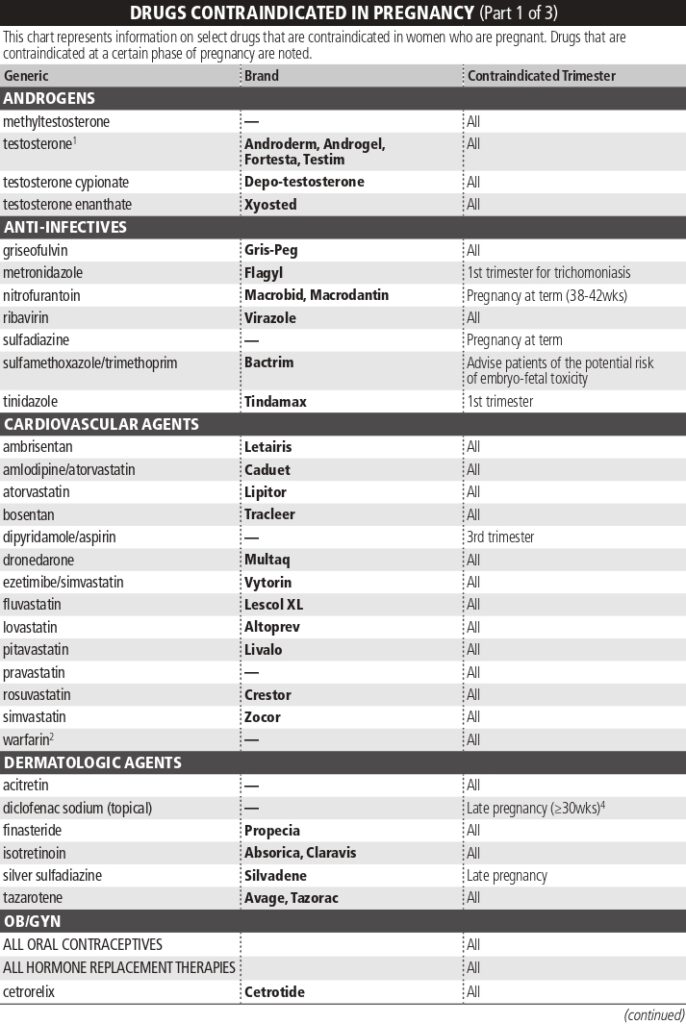
Some of these agents are easy to avoid. Others may be required for a medical condition and are unavoidable. For instance, you may require phenytoin to control your seizures if you’re pregnant and you have epilepsy. Despite the risk of teratogenic effects, you may be better off taking the phenytoin than risking the occurrence of uncontrolled seizures during pregnancy.
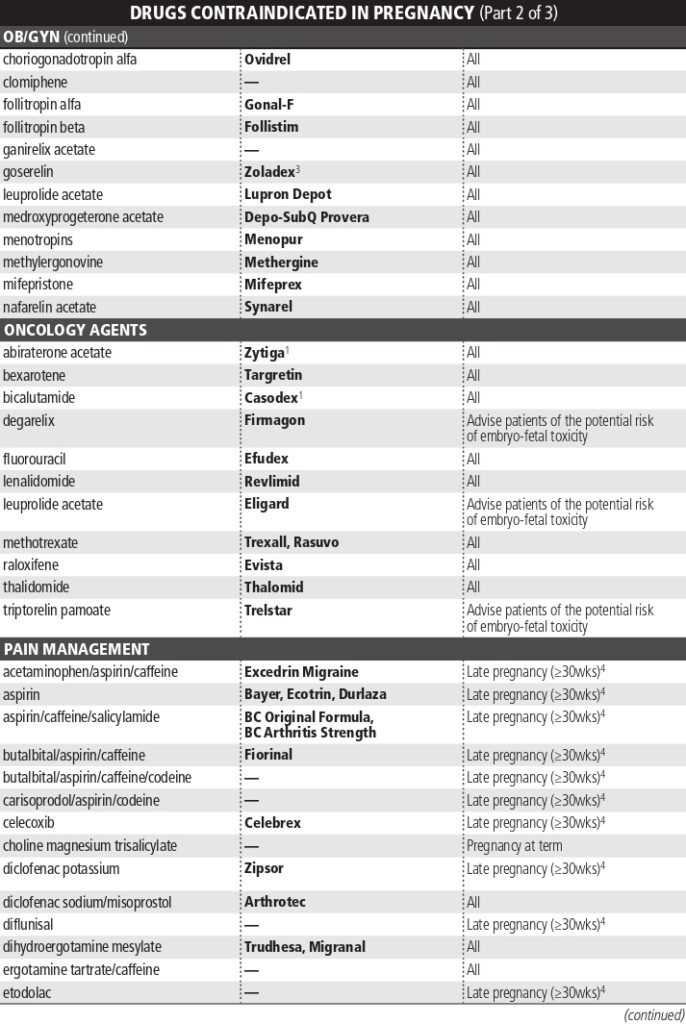
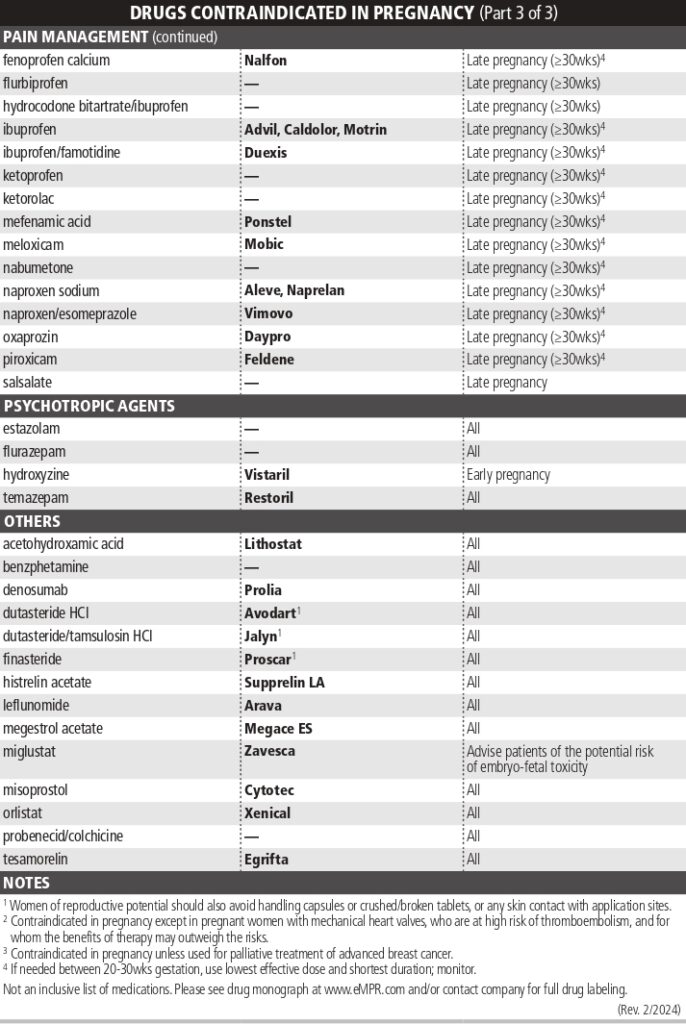
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
such as Advil (ibuprofen), Aleve (naproxen), and Ecotrin (aspirin)—help reduce pain, inflammation, and fever. NSAIDs can cause serious kidney problems in a fetus, especially after 20 weeks (5 months) of gestation. After 20 weeks, the fetus’s kidneys produce most of the protective amniotic fluid surrounding the fetus, which is essential for developing the lungs, muscles, and digestive system.
While NSAID use is most dangerous after 20 weeks of pregnancy, you may want to avoid the drugs throughout your entire pregnancy. Some evidence suggests NSAIDs increase the risk of miscarriage and birth defects when taken in early pregnancy.
Statins (Drugs that can lower cholesterol)
Statins such as
- Atorvastatin (Caduet ® or Lipitor ® ).
- Fluvastatin.
- Lovastatin (Mevacor ® or AltoprevTM).
- Pitavastatin
are prescription medications that lower blood cholesterol levels in people with high cholesterol. They work by reducing cholesterol production in the liver and helping the liver remove low-density lipoprotein (LDL)—bad cholesterol—from the blood.
In 2021, the U.S. Food and Drug Administration (FDA) removed the strongest warning against statin use during pregnancy after acknowledging research evidence that shows statins do not cause birth defects. However, statins are associated with other risks during pregnancy, including a higher risk of low birth weight and preterm birth.
Retinoids
Retinoids, such as Zenatane (isotretinoin), are prescription acne medications associated with a high risk of severe birth defects. These medications affect how cells grow and divide, disrupting the normal development of an embryo or fetus. Retinoid use during pregnancy is associated with malformations (e.g., cleft lip or palate; abnormal head shape), heart defects, intellectual disabilities, and developmental delays.
Although oral retinoids are particularly dangerous for a fetus, there is not enough research to determine whether topical retinoids (creams and lotions) are safe. Some experts recommend avoiding them entirely during pregnancy.
Warfarin (Blood Thinner)
Blood thinners, or anticoagulants, are prescription medications that help prevent blood clots. Coumadin (warfarin) is a blood thinner that passes through the placenta to the fetus and increases the risk of miscarriage, stillbirth, and congenital disorders.
Warfarin use in the first trimester is associated with fetal warfarin syndrome (FWS), which causes skeletal problems such as shortened limbs, skull and facial differences, intellectual disability, and heart defects.
In the second and third trimesters, warfarin use increases the risk of hemorrhage (excessive bleeding) and stillbirth. Fortunately, there are blood thinners that are safe to take during pregnancy, such as heparin, that do not pose health risks to a developing fetus.
Anti-Seizure Medications
Anti-seizure medications (ACMs) help reduce the frequency of seizures in people with seizure disorders, such as epilepsy.
Some ACMs, particularly Valproic (valproic acid), increase the risk of congenital disorders. Valproic acid exposure in the first trimester is associated with a high risk of babies born with neural tube defects, such as spina bifida, cleft lip, and heart defects. Exposure in the first trimester is also associated with an increased risk of intellectual disabilities, autism spectrum disorder, facial differences, and limb defects.
The decision of whether or not to take ACMs during pregnancy involves weighing the risks of uncontrolled seizures for both the pregnant parent and fetus against the potential birth risks. Your healthcare provider can advise you based on your specific health needs.
Tetracycline Antibiotics
Tetracyclines, such as Monodox (doxycycline), are antibiotics that treat many bacterial infections, including respiratory tract infections and skin, eye, intestinal, and urinary tract infections.
During pregnancy, these medications can affect bone growth and cause permanent staining of a baby’s teeth. While less common, tetracycline may slow bone growth in the developing fetus. However, this effect appears to be reversible once the pregnant parent stops taking the medication.
High-dose tetracyclines also pose a health risk for pregnant people, increasing the risk of acute fatty liver in pregnancy (AFLP), a rare but possibly life-threatening disorder. Healthcare providers can prescribe safer antibiotics to treat bacterial infections during pregnancy.
Benzodiazepines
Benzodiazepines (like Valium) are sedative medications that treat anxiety and insomnia. Some studies suggest a possible link between first-trimester exposure to benzodiazepines and an increased risk of heart problems. The risk may be dose-dependent, meaning a higher dose could lead to a greater risk.
Long-term use of benzodiazepines throughout pregnancy may affect the developing fetus’s central nervous system and increase the risk of preterm birth and low birth weight. Newborns exposed to benzodiazepines may experience respiratory distress, low muscle tone, and poor feeding and require admission to the neonatal intensive care unit (NICU).
Decongestants
Decongestant medications containing Sudafed (pseudoephedrine) can help relieve nasal congestion from allergic rhinitis (hay fever).
Some evidence suggests there is a link between pseudoephedrine use in the first trimester and an increased risk of congenital disorders, including gastroschisis (an opening in the abdominal wall), small intestinal atresia (underdeveloped small intestine), and hemifacial microsomia (smaller than usual facial features).
Pseudoephedrine acts as a vasoconstrictor, meaning it narrows blood vessels. This may reduce blood flow to the uterus and fetus, especially during the first trimester when organ formation occurs.
ACE Inhibitors
Angiotensin-converting enzyme (ACE) inhibitors, such as Lotensin (benazepril) and Zestril (lisinopril), are prescription medications that treat hypertension (high blood pressure), heart disease, and kidney problems.
MedlinePlus. ACE inhibitors.
These medications pose potentially serious risks for a fetus, particularly in the second and third trimesters. ACE inhibitors can cause low levels of amniotic fluid in the womb, increasing the risk of congenital disorders, including lung and kidney problems, skull deformities, and, in severe cases, fetal death.
Methotrexate
Trexall (methotrexate) is a medication that blocks the growth of cells and decreases immune system activity to treat autoimmune conditions like rheumatoid arthritis and certain types of cancer. Methotrexate poses serious risks during pregnancy. Exposure in the first trimester is associated with congenital anomalies such as craniofacial (face and skull), finger and toe, and spinal defects.
Exposure to methotrexate in the first trimester also increases the risk of lung, heart, and kidney problems. Studies suggest that low-dose methotrexate may increase the risk of miscarriage, preterm birth, or intrauterine growth restriction (IUGR) that may stunt growth through infancy and childhood.
Cannabis
Cannabis (marijuana) is a plant that some people use to treat anxiety, insomnia, nausea, and pain. Cannabis contains tetrahydrocannabinol (THC), a psychoactive compound that crosses the placenta and affects fetal development.
Smoking, vaping, or ingesting cannabis edibles during pregnancy can lead to adverse outcomes such as low birth weight, preterm birth, and developmental delays. Some studies suggest the effects may continue throughout childhood—some children whose gestational parents used cannabis while pregnant have behavioral and learning problems.
Lithium
Lithium, a mood-stabilizing prescription medication for treating bipolar disorder, poses potential risks during pregnancy. First-trimester lithium exposure increases the risk of heart defects in developing fetuses, such as Ebstein anomaly, which affects the positioning and function of a heart valve.
Some studies suggest lithium use during pregnancy may increase the risk of preterm birth and low birth weight, though the risk appears to be small. However, lithium use is associated with neonatal complications, such as respiratory distress, poor feeding, and low muscle tone, requiring longer hospital stays after birth.
Many people with bipolar disorder who take lithium during pregnancy deliver healthy babies. However, your healthcare provider may recommend lowering your lithium dose to prevent adverse outcomes. Talk to your provider before stopping or reducing your medication.
Opioids
Opioids, such as buprenorphine, codeine, and oxycodone, are powerful pain medications that help manage moderate to severe pain. Opioid use during pregnancy is associated with an increased risk of miscarriage, stillbirth, and congenital disorders, including heart defects, neural tube defects (e.g., spina bifida), and eye problems like glaucoma and blindness.
Opioid exposure can lead to neonatal abstinence syndrome (NAS) when a baby goes through withdrawal from the drug after birth. Babies with NAS may cry excessively, have body shakes or seizures, breathing problems, diarrhea, fever, or have trouble eating and gaining weight.
High Doses of Vitamins
Prenatal vitamins are important for a healthy pregnancy, but excessive intake of certain vitamins may be unsafe during pregnancy, especially in high doses. For example, excessive intake of vitamin A during pregnancy increases the risk of birth defects and miscarriage.
Also, high doses of vitamin E during pregnancy are associated with an increased risk of intrauterine growth restriction, premature rupture of membranes (water breaking early), placental abruption, preterm birth, and stillbirth.