Wisdom Tooth: Cause, Indication and Contraindications
Explore the Orthodontic theory of impaction, where jaw development and movement play a crucial role. how dental arches can lead to impaction.

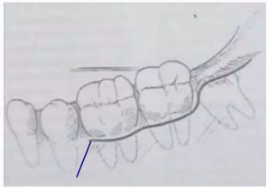

Explore the Orthodontic theory of impaction, where jaw development and movement play a crucial role. how dental arches can lead to impaction.

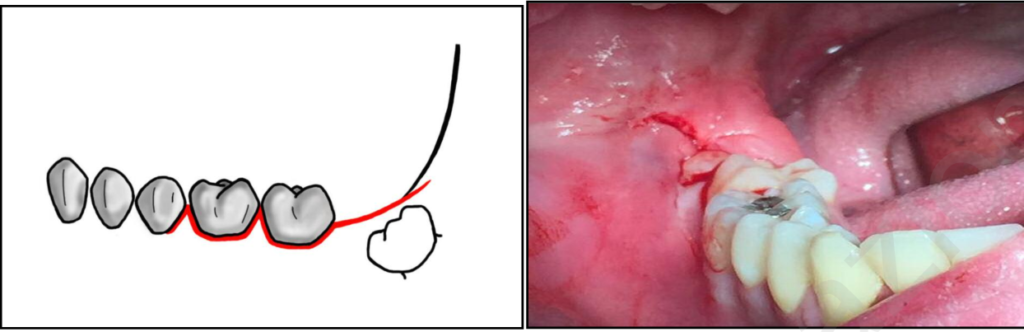
Discover the various techniques of bone removal for impacted teeth on our website. find out the best methods for successful tooth extraction.