Wisdom Tooth: Investigation and Examinatio
Don’t let tooth impaction affect your quality of life. understand the causes, symptoms, and treatment options for impacted teeth.


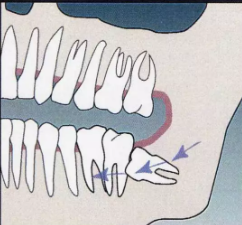
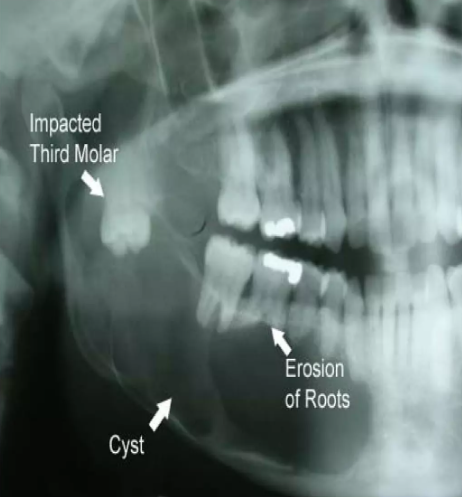

Don’t let tooth impaction affect your quality of life. understand the causes, symptoms, and treatment options for impacted teeth.

Understand the steps involved in creating this flap design for improved access and visibility during surgical procedures.