(Previously known as Chronic Apical Periodontitis)
Introduction
Asymptomatic apical periodontitis is a type of apical periodontitis that does not produce any clinical signs or symptoms. However, long-term inflammation can eventually destroy the tissue surrounding the teeth. Asymptomatic apical periodontitis is an inflammation and destruction of the apical periodontium. It appears as an apical radiolucent area and does not produce clinical symptoms. Unlike their acute counterparts, chronic lesions are often asymptomatic—a chronic, low-grade defensive reaction of the alveolar bone to the irritation from the root canal. During a later stage of disease progression, the tooth becomes loose or may be lost.
Causes
- Chronic periodontitis involves an imbalance between the commensal microbiota and the host defence.
- Asymptomatic apical periodontitis is caused by the death of the pulp, followed by a mild infection or irritation of the periradicular tissue.
- Chronic or asymptomatic infections may initiate and modulate the intravascular accumulation of inflammatory cells, resulting in endothelial dysfunction, which subsequently represents a possible systemic inflammatory burden.
- The accumulation of microorganisms in dental biofilms causes inflammation of the adjacent gingiva (gingivitis), resulting in the destruction of tooth-supporting tissue.
Symptoms
- Asymptomatic apical periodontitis may not produce any subjective reactions.
- In rare cases, it breaks down and undergoes suppuration.
- The pulp is necrotic and infected; therefore, pulp sensibility tests will not elicit a response.
- The tooth is not tender to palpation, pressure, or percussion.
- The tooth may have some mobility and feel different.
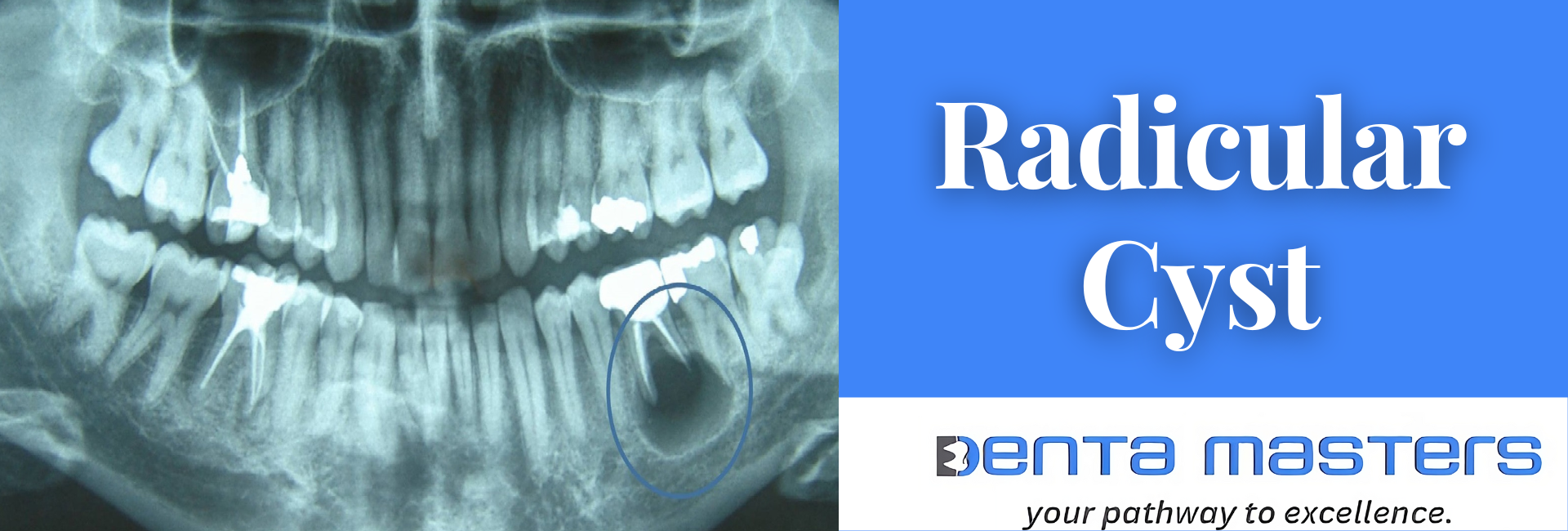
Diagnosis
- Diagnosis is generally done by routine radiographic examinations.
- Assessment of the level of alveolar bone in the radiograph.
- The area of rarefaction is well defined, with a lack of continuity in the lamina dura.
- The methods used in clinical practice are probing of the periodontal pocket to record bleeding on probing and to measure the pocket depth.
- The absence of bleeding on probing of periodontal pockets that had previously been inflamed indicates that treatment had led to an improvement in periodontal health.
Differential Diagnosis
- Asymptomatic apical periodontitis cannot be differentiated from other periradicular diseases unless the tissue is examined histologically.
- A necrotic pulp and a periapical area of rarefaction on a radiograph are usually sufficient evidence of the presence of periradicular disease.
- The periradicular diseases are all treated alike, usually endodontically, and do not have to be differentiated.
- Apical Radiolucencies
- Periapical granuloma
- Periapical cyst
- Lateral periodontal cyst
- Dentigerous cysts
- Odontogenic keratocysts
- Ameloblastomas
- Apical Radiopacities
- Hypercementosis
- Cemento-osseous dysplasia
- Idiopathic osteosclerosis
- Apical radiopacities are likely not associated with endodontic infection directly but are commonly found on routine radiographic evaluation. Radiopacities are generally benign.
Bacteriology
- Bacteriologic examination of the periradicular tissues has shown that bacteria, although found in the apical area of the root canal, are seldom present in the periradicular area.
- The periapical tissue is sterile in most cases.
Histopathology
- Granulomatous tissue replaces the alveolar bone and periodontal ligament.
- It consists of an outer fibrous capsule, which is continuous with the periodontal ligament, and an inner or central portion made up of loose connective tissue and blood vessels.
- It is composed of a rich vascular network, fibroblasts derived from the periodontal ligament, and a moderate infiltration of lymphocytes and plasma cells.
- As the inflammatory reaction continues, because of irritation from bacteria or their products, the exudate accumulates at the expense of the surrounding alveolar bone.
- This process is followed by the clearing of the dead osseous tissue by macrophages, or foreign-body giant cells, while at the periphery, fibroblasts actively build a fibrous wall.
- The alveolar bone at the periphery of the lesion may show resorption, and osteoclasts may be present.
- The root surface may show external root resorption due to cementoclastic activity or hypercementosis due to cementoblast activity.
Treatment
- Treatment aims to remove or significantly reduce the intracanal microbes and prevent re-infection by placing a root canal filling.
- Root canal therapy may suffice for the treatment of asymptomatic apical periodontitis.
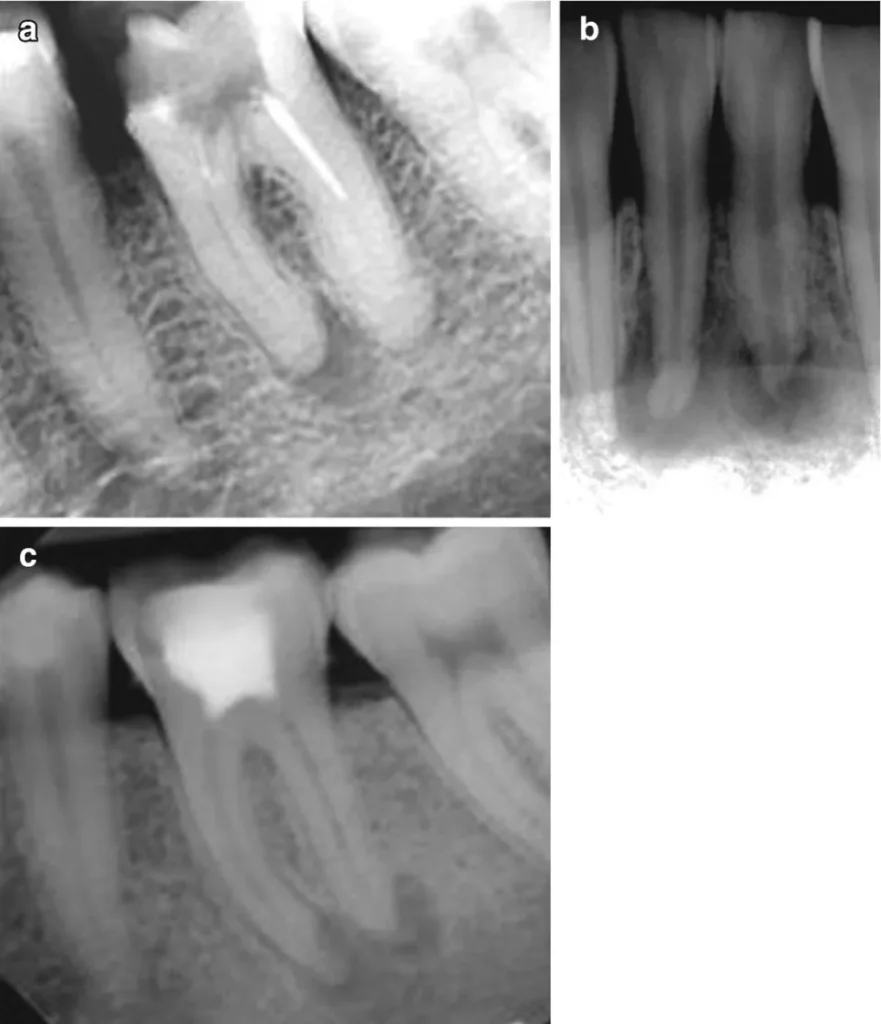
- When endodontic treatment is adequately done, the periapical lesion heals with hard tissue regeneration, which is evident in follow-up radiographs through a reduction in the radiolucency’s size.
- Apical periodontitis lesions are expected to heal completely within six months to two years, but some may persist.
- Removal of the cause of inflammation is then followed by resorption of the granulomatous tissue and repair with trabeculated bone.
- Further management is indicated when a periapical radiolucency remains unchanged after one year of root canal treatment, increases in size, or appears in an endodontic-treated tooth without a prior apical disease.
- Some periapical lesions may persist despite following the most strict and careful clinical protocol due to the complex anatomy of the root canal system.
- Antibiotic use is generally contraindicated, except in cases of rapid onset or systemic involvement. These cases include lymphadenopathy, malaise, a sudden onset of symptoms in less than 24 hours, and a fever over 38 degrees Celsius.
- Despite not being used in every case, antibiotics may be necessary for immunocompromised patients.
Prognosis
The prognosis for long-term retention of the tooth is excellent.