Table of Contents
Habit
- A habit can be defined as “a constant settled practice or custom, established by the repetition of the same act.”. It is a tendency towards an act that has become a repeated performance, relatively fixed, consistent, and easy to perform by an individual.
- Oral habits are repetitive behaviours in the oral cavity that can have significant impacts on dental and facial development. These habits, if persistent, can lead to various malocclusions and other orthodontic problems.
Classification of Oral Habits
- Useful Habits vs. Harmful Habits
- Empty Habits vs. Meaningful Habits
- Pressure Habits vs. Non-Pressure Habits
- Biting Habits vs. Compulsive Habits vs. Non-Compulsive Habits
- Nutritive vs. Non-Nutritive Habits
- Daytime vs. Nighttime Habits
- Self-Inflicted vs. External Habits
- Intermittent vs. Continuous Habits
1. Useful Habits vs. Harmful Habits
- Useful habits: Habits that do not cause any adverse effects on dental and facial developments. These encompass examples including normal deglutition, normal respiration, etc.
- Harmful habits: Habits that can lead to malocclusions and other orthodontic problems. These encompass examples including thumb sucking, nail biting, etc.
2. Empty Habits vs. Meaningful Habits
- Empty habits: habits that serve no specific purpose and are performed without any underlying need or motivation, for example, placing the tongue in a certain position.
- Meaningful habits: Habits that fulfil a specific need or purpose, such as self-soothing or coping with stress example mouth breathing, tongue thrusting, etc.
3. Pressure Habits vs. Non-Pressure Habits
- Pressure habits: Habits that exert direct pressure on the teeth, jaws, or surrounding structures, such as thumb sucking or tongue thrusting.
- Non-pressure habits: Habits that do not directly apply pressure, such as lip biting or nail biting
4. Biting Habits vs. Compulsive Habits vs. Non-Compulsive Habits
- Biting habits: Habits involving biting or chewing on objects, such as nails, lips, or cheeks.
- Compulsive habits: Habits that are repetitive, uncontrollable, and difficult to break, such as hair pulling or skin picking.
- Non-compulsive habits: Habits that are not as deeply ingrained or difficult to break, such as thumb sucking or tongue thrusting.
5. Nutritive vs. Non-Nutritive Habits
- Nutritive habits: habits involving the consumption of food or liquids, such as chewing gum or frequent snacking. These habits may have implications for dental health and occlusal function.
- Non-nutritive habits: habits that do not involve the intake of food or liquids, such as thumb sucking or tongue thrusting. These habits can lead to malocclusions and other orthodontic issues.
6. Daytime vs. Nighttime Habits
- Daytime habits: habits that occur during waking hours, such as nail biting or lip biting. These habits may be more noticeable and easier to address through conscious effort.
- Nighttime habits: habits that occur during sleep, such as bruxism (teeth grinding) or mouth breathing. These habits can be more challenging to control and may require specialised interventions.
7. Self-Inflicted vs. External Habits:
- Self-inflicted habits: Habits that individuals engage in voluntarily, such as nail biting or lip biting. These habits are within the individual’s control and may be influenced by psychological factors.
- External habits: Habits that are triggered or reinforced by external stimuli, such as environmental stressors or peer influence. These habits may require environmental modifications or behavioural interventions.
8. Intermittent vs. Continuous Habits
- Intermittent habits: Habits that occur sporadically or in response to specific triggers, such as stress or boredom. These habits may vary in frequency and intensity over time.
- Continuous habits: Habits that are ongoing and persistent, with little variation in frequency or duration. These habits may have a more pronounced impact on dental and facial development
The types of habits
- Thumb Sucking
- Chewing on Hard Objects
- Tongue Thrust
- Grinding/Clenching:
- Lip or Nail Biting
- Mouth Breathing
Thumb Sucking

Effects of thumb sucking:
- Thumb-sucking exerts continuous pressure on the developing teeth, causing them to shift from their normal position.
- Prolonged and forceful thumb-sucking can result in dental misalignment, leading to malocclusion, where the upper and lower teeth do not fit together correctly.
- Malocclusion can affect speech, chewing, and overall oral health.
Clinical features -
The clinical features of the thumb sucking habit in orthodontics include:
- Anterior Open Bite: Prolonged thumb sucking can lead to an anterior open bite, where there is a lack of vertical overlap between the upper and lower front teeth.

- Exaggerated Overjet: Thumb sucking may contribute to an exaggerated overjet, where the upper front teeth protrude significantly beyond the lower front teeth.

- Posterior Crossbite: This habit can result in a posterior crossbite, where the upper teeth fit inside the lower teeth when the jaws are closed.

- Retrognathic Mandible: Thumb sucking can lead to a retrognathic mandible, where the lower jaw is positioned further back than normal.

- Diastema: The habit may cause a diastema, which is a gap between teeth, particularly in the front teeth area.

Prevention
- Early Intervention:
- Addressing the habit as early as possible, ideally before the eruption of permanent teeth, to prevent potential orthodontic issues.
- Parental Guidance:
- Educating parents on the adverse effects of thumb sucking and providing strategies to help their child break the habit effectively
Treatment
- Behavioural Modification Techniques:
- Positive Reinforcement: Encouraging and rewarding the child for not sucking their thumb can be effective in breaking the habit.
- Counselling Sessions: Providing guidance and support to the child to understand the reasons behind the habit and how to overcome it.
- Time-Out Strategy: Removing a reinforcer whenever thumb-sucking occurs, such as stopping a preferred activity when the habit is noticed.
- Competing Response Therapy: Introducing an alternative behaviour, like squeezing an object, whenever the child feels the urge to suck their thumb.
- Orthodontic Appliances:
- Habit-Breaker Appliances: Devices designed to obstruct thumb sucking and make it more challenging to continue the habit. These appliances can help in breaking the habit and preventing further dental issues. The example of a habit-breaking appliance is a custom-made device. This device prevents the placement of the thumb into the mouth comfortably and soothingly. Thus it is used to break a persistent thumb sucking habit in a child or adult.
- Negative or Aversion Therapies:
- Foul-Tasting Substances: Applying a foul-tasting oil on the thumb can create an aversion to thumb sucking.
- Physical Barriers: Using gloves, bandages, or nail polish to remind the child not to put their thumb in their mouth.
- Dental Appliances:
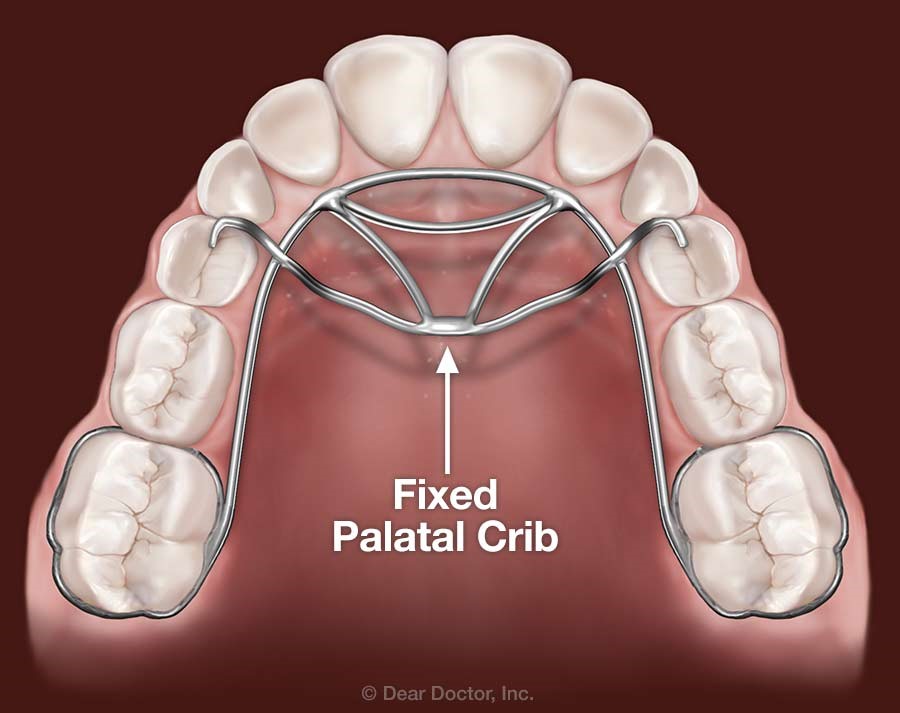
- Palatal Crib (Vertical Crib/Tongue Crib: A dental appliance that has been successful in treating thumb sucking habits by creating a physical barrier to discourage the habit.
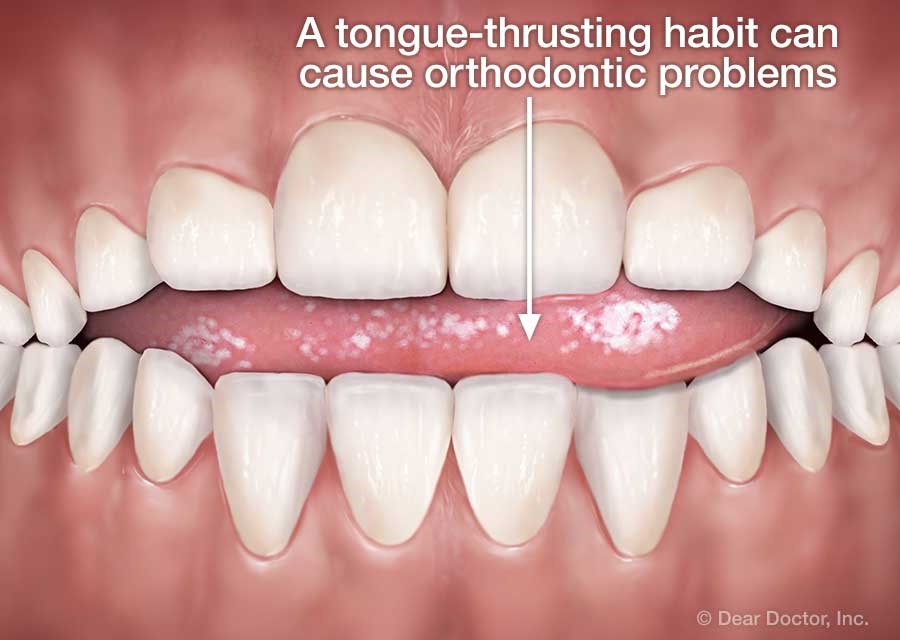
Tongue Thrusting
- Tongue thrust appears when the tongue presses forward too far in the mouth, resulting in an abnormal orthodontic condition called an “open bite.
- The condition is most common in children.
- It has a myriad of causes, including:
- poor swallowing habits
- allergies
- tongue-tie
Clinical features
The clinical features of tongue thrusting habit in orthodontics include:
- Extra-oral Features:
- Greater lip separation: The gap between the upper and lower lip is larger than normal.
- Erratic movement of the lower jaw during swallowing.
- Speech disorders: Such as lisping and sibilant distortions. (Lisping is a speech disorder wherein the patient is unable to correctly pronounce the sounds of s or z.)
- Pronunciation problems: Difficulty in pronouncing certain sounds like s, n, t, d, l, th, v, z.
- Greater anterior facial height than normal.
- Intra-oral Features:
- Jerky and irregular swallowing sequences.
- Increased proclination of upper front teeth.
- Greater spacing between the teeth.
- Retroclination or proclination of lower front teeth.
- Decreased width of the upper jaw.
- Anterior or posterior open bite due to the space created by the tongue between the teeth.
- Posterior crossbite.
Prevention Strategies
- Early Intervention:
- Addressing the habit as early as possible, ideally before the eruption of permanent teeth
- Parental Guidance:
- Educating parents on the adverse effects of tongue thrusting and providing strategies (as mentioned under treatments) to help the child break the habit
- Self-Motivation:
- Encouraging the child to want to stop the habit by explaining the benefits and building self-esteem
- Physical Barriers:
- Using devices like tongue cribs or other appliances to discourage the tongue thrusting behaviour
- Addressing Underlying Causes:
- Treating any underlying issues like allergies, enlarged tonsils, or tongue-tie that may contribute to the development of the habit
Treatment
- Behavioural Modification Techniques:
- Positive reinforcement
- Counselling sessions
- Time-out strategy
- Competing response therapy
- Orthodontic Appliances:
- Tongue crib/habit-breaker appliancesIt physically blocks the tongue from going between the teeth. By preventing tongue thrusting habit, it allows proper positioning of the tongue and swallowing patterns to develop.
- Palatal crib (vertical crib/tongue crib)This appliance has vertical wires. The wires extend from the palatal acrylic plate to the incisal edges of the anterior teeth. It thereby restricts the tongue from pushing forward and breaks the tongue thrusting habit.
- Orofacial Myofunctional Therapy:
- Exercises to retrain and correct tongue positioning
It involves exercises to retrain and correct tongue positioning, which eventually help break the habit of tongue thrusting and promote proper swallowing patterns. These exercises include:- Touching the tongue tip to the area just behind the upper front teeth (alveolar ridge) helps train proper tongue positioning during swallowing.
- Pressing the tongue firmly against the palate and holding for several seconds, then releasing. This helps strengthen tongue muscles and promotes proper tongue posture.
- Lip sealing: In this exercise, lips are closed together tightly and held for several seconds, then released.
- Cheek puffing: Puffing out the cheeks and holding the air in, then releasing. This exercise helps strengthen the cheek muscles and encourages proper cheek support during swallowing.
- Exercises to retrain and correct tongue positioning
- Orthodontic Treatment:
• Braces or Invisalign: These help in the correction of dental misalignment caused by tongue thrusting

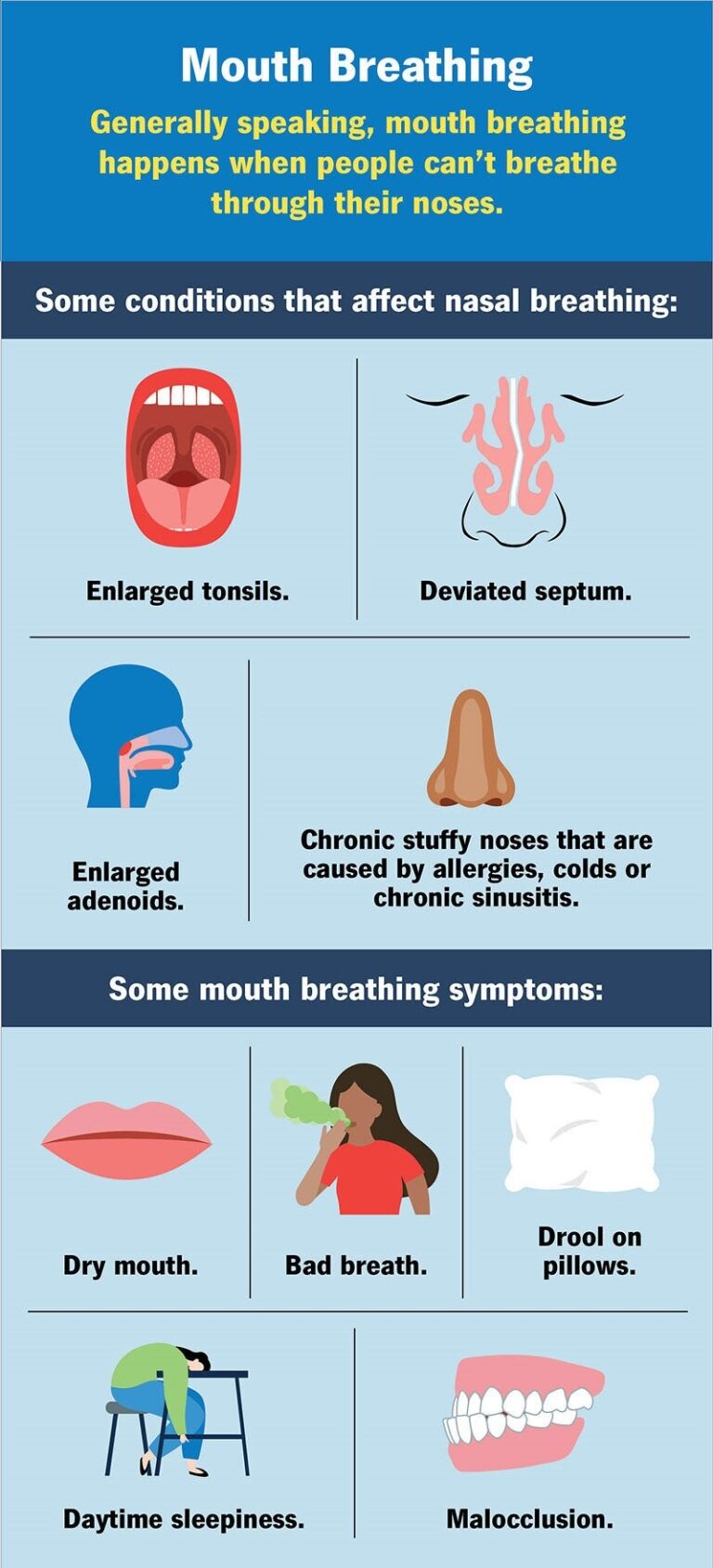
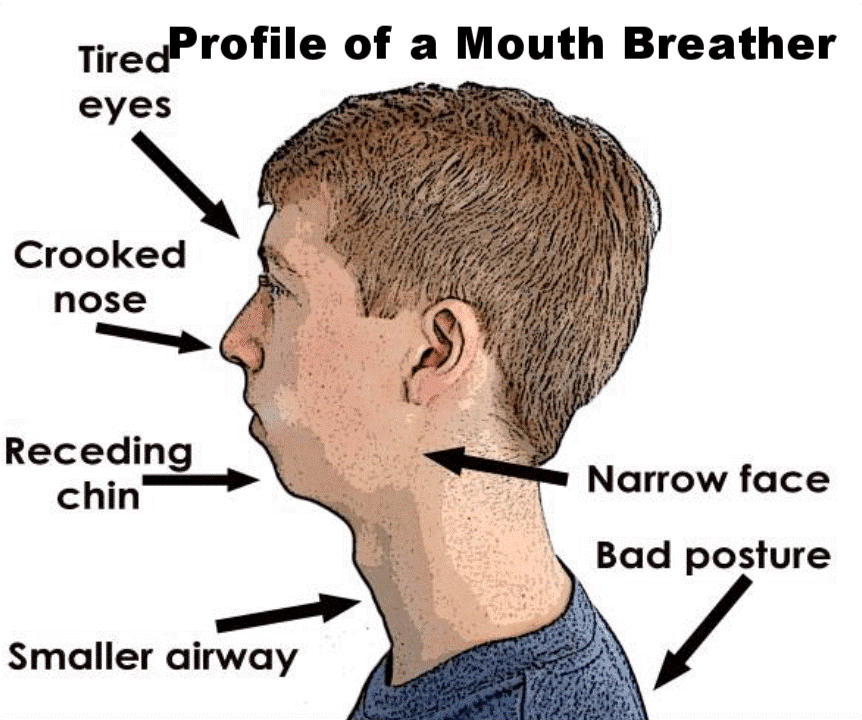
Mouth Breathing
- Mouth breathing is when people can’t breathe through their nose so they take in air through their mouths.
- Mouth breathing can cause sleep disorders that affect daily life. It also can change the structure of people’s faces.
Causes
Mouth breathing happens when people can’t breathe through their noses. Some conditions that affect nasal breathing include:
- Enlarged adenoids: Adenoids are glands that look like small lumps of tissue located above the roof of the mouth and behind the nose. Adenoids protect young children from bacteria and viruses. Sometimes, these are swollen or infected, blocking children’s airways. Adenoids typically shrink as people age, so enlarged adenoids are less likely to cause mouth breathing in adults.
- Nasal congestion: If the patient have allergies, colds or chronic sinusitis, they may have a persistent stuffy nose that keeps them from breathing through their nose.
- Deviated septum: Septum is a cartilage and bone that divides the inside of the nose into two sides. When the septum leans to one side, it can block the airway.
Clinical features
key clinical features of the mouth breathing habit in orthodontics include:
- Extra-Oral Features:
- Facial form: long, narrow face (dolicofacial)
- Increased anterior facial height
- Increased mandibular plane angle
- Slack, open, and everted lower lip
- Lip-apart posture
- Class two-type malocclusion
- Intra-Oral Features:
- Proclination and spacing of anterior teeth
- Constricted maxillary arch and posterior crossbites
- Decreased vertical overlap of anterior teeth
- Inflamed gingival tissue in the upper anterior region
- Other Clinical Features:
- Adenoid facies: long, narrow face, short upper lip, anteriorly placed nares, narrow maxilla
- Hoarseness of voice
- Repeated respiratory infections and allergic rhinitis
- Otitis media (middle ear infections)
- Increased caries incidence
- More visible plaque and calculus are seen in mouth breathers than in nasal breathers
Prevention strategies
- Early Intervention:
- Identifying and addressing mouth breathing habits in children as early as possible to prevent long-term consequences on facial and dental development.
- Parental Guidance:
- Educating parents and children about the importance of nasal breathing and the negative effects of chronic mouth breathing on oral and overall health.
- Self-Motivation:
- Encouraging the child to want to stop the habit by explaining the benefits and building self-esteem.
- Physical Barriers:
- Using devices like oral screens or other appliances to discourage mouth breathing and promote nasal breathing.
Treatment Modalities
- Nasal Airway Assessment:
- Evaluation by an otolaryngologist to assess and address any nasal obstructions or issues that may be causing mouth breathing.
- Myofunctional Therapy:
- Orofacial exercises to retrain the muscles of the face and mouth for proper breathing through the nose.
- Orthodontic Treatment:
- Correction of dental and skeletal issues resulting from mouth breathing, such as expansion of the maxilla or correction of malocclusions.
- Allergy Management:
- Treatment of allergies or sinus issues that may contribute to nasal congestion and mouth breathing.
- Breathing Exercises:
- Techniques to promote nasal breathing and discourage mouth breathing, such as pursed lip breathing and diaphragmatic breathing
Orthodontic Appliances Used in Treating Mouth Breathing
- Oral Screen: An appliance used to re-establish nasal breathing and prevent mouth breathing, particularly in mouth breathers
- Pre-Orthodontic Trainer: Utilised in children with mouth breathing habits to help correct the breathing pattern and promote nasal breathing.
- Mandibular Anterior Repositioning Appliance (MARA): A functional appliance used in the treatment of Class II malocclusions which are caused by prolonged mouth breathing. This appliance addresses malocclusion issues related to mouth breathing


Bruxism
- Bruxism is a harmful oral habit in orthodontics. It is characterised by typical involuntary, excessive grinding or clenching habit of the teeth.
- It mostly occurs during sleep (sleep bruxism). It can also be seen while patient is awake (awake bruxism).
- Bruxism is a multifactorial habit or condition that might get triggered by physical, psychological, or genetic factors.
- If it is not treated on time, it can lead to damaged teeth, jaw disorders, and other dental problems
Clinical features


- Dental Wear and Damage:
- Excessive wear and damage to the tooth enamel and underlying structures due to the grinding and clenching of teeth.
- Sensitivity and pain in the teeth
- Temporomandibular Joint (TMJ) Issues:
- Clicking, popping, or grinding sounds in the TMJ.
- Pain and discomfort in the jaw joint and surrounding muscles.
- Limited range of motion in the jaw.
- Muscle Hypertrophy:
- Enlargement and increased tone of the masticatory muscles, such as the masseter and temporalis muscles.
- Orthodontic Implications:
- Ineffectiveness or relapse of orthodontic treatment due to the destructive forces of bruxism.
- Increased risk of tooth fractures, loosening, or loss during orthodontic treatment.
- Sleep Disturbances:
- Bruxism is often associated with sleep disorders, such as sleep apnoea, which can further impact overall health and well-being.
Preventive Measures
- Dental Correction:
- If certain dental issues are causing bruxism, restorative procedures like crowns can restore tooth shape and function.
- Orthodontic treatments can realign teeth, reducing strain on the jaw.
- Stress Management
- Identifying stress-causing factors and reducing them can help decrease bruxism episodes.
- Practice relaxation techniques like yoga and deep breathing to lower stress levels.
- Behavioural Therapies:
- Cognitive Behavioural Therapy (CBT) can help change thought patterns leading to stress and bruxism.
Treatment Modalities
- Orthodontic Treatment:
- Fixing bite problems and aligning the teeth and jaws can help prevent or reduce bruxism.
- Orthodontic treatment can address the underlying malocclusions that may be contributing to the bruxism habit.
- Occlusal Splints/Night Guards:
- Maxillary night guards that keep all the teeth in contact can be effective in managing bruxism.
- These appliances protect the teeth from the destructive forces of grinding and clenching.
- Muscle Relaxation Techniques:
- Exercises and therapies to relax the masticatory muscles, such as the masseter and temporalis, can help reduce bruxism.
- Stress Management:
- Addressing underlying psychological factors, such as anxiety and stress, through counselling or relaxation techniques.

Orthodontic Appliances Used for Bruxism Treatment
- Maxillary Night Guards:
- These occlusal splints are designed to fit over the upper teeth and keep the teeth in contact, preventing direct tooth-to-tooth contact during grinding.
- Mandibular Advancement Devices:
- These appliances position the lower jaw slightly forward, which can help reduce the intensity of bruxism episodes.
- Anterior Bite Plates:
- Appliances that create an anterior open bite prevent posterior tooth contact and reduce the forces of bruxism.
- Palatal Expanders:
- In some cases, expanding the maxillary arch can help improve the occlusal relationship and reduce bruxism.
Lip Biting
Habit of biting the lips, whether voluntarily or involuntarily.
Causes
- Physical causes:
- In some cases, physical conditions can cause a person to bite their lips when they use their mouth for talking or chewing. Physical causes of lip biting include:
- Teeth alignment issues, known as malocclusion. These include overbite and underbite, which can lead to overcrowding of the teeth.
- Temporomandibular disorder, or TMD, is a condition that affects the chewing muscles. People with malocclusion or TMD may often bite their lips, cheeks, or tongue. Treatment options can be recommended, which may include dental braces or removing one or more teeth.
- Psychological causes:
- People may bite their lips as a physical response to an emotional state, such as stress, fear, or anxiety.
- Chronic lip biting is one example of a body-focused repetitive behaviour, or BFRB. This term refers to any repetitive, self-directed behaviour that damages the skin, hair, or nails.
- BFRBs occur as a coping mechanism in situations where a person is feeling uncomfortable or anxious. People with a BFRB find that repetitive behaviours can provide relief from painful emotions.
Clinical features
key clinical features of the lip-biting habit
- Lip Deformation:
- The lower lip may slide in behind the upper teeth, causing pressure on the upper teeth.
- This can lead to the development of an overbite, where the upper teeth protrude excessively over the lower teeth.
- Dental Crowding:
- The constant pressure and force exerted on the teeth by lip-biting can cause the teeth to become crowded and misaligned over time.
- Dry and Chapped Lips:
- Repeated biting and chewing on the lips can cause the lips to become dry, cracked, and chapped.
- Soft Tissue Damage:
- Constant trauma to the lip tissue can lead to inflammation, swelling, and the development of lesions or sores on the lips.
- Speech Difficulties:
- In some cases, the lip deformation and dental crowding caused by lip biting can lead to speech problems, such as difficulty pronouncing certain sounds.
- Psychological Factors:
- Lip-biting is often associated with underlying psychological factors, such as stress, anxiety, or a desire for attention.
Based on the information provided in the search results, the prevention, treatment, and orthodontic appliances used for the management of oral habits in orthodontics can be summarised as follows:
Prevention
- Early Intervention:
- Identifying and addressing oral habits, such as thumb sucking or tongue thrusting, as early as possible to prevent long-term consequences.
- Parental Guidance:
- Educating parents on the adverse effects of oral habits and providing strategies (like mentioned under treatments) to help the child break the habit.
- Promoting Healthy Habits:
- Encouraging good oral hygiene, proper breathing, and healthy lifestyle habits to support overall oral and facial development.
Treatment
- Behavioural Modification Techniques:
- Positive reinforcement, counselling sessions, time-out strategies, and competing response therapy can help the child break the habit.
- Orthodontic Appliances:
- Habit-breaker appliances, such as palatal cribs or tongue cribs, to physically discourage the habit.
- Mandibular Anterior Repositioning Appliance (MARA) to address issues related to mouth breathing.
- Occlusal splints or night guards to manage bruxism (teeth grinding).
- Myofunctional Therapy:
- Orofacial exercises to retrain the muscles and correct improper oral habits, such as tongue thrusting or mouth breathing.
- Addressing Underlying Causes:
- Treatment of any underlying issues, such as allergies or nasal obstructions, that may be contributing to the development of oral habits.
- Shahraki N, Yassaei S, Moghadam MG. Abnormal oral habits: A review. J Dent Oral Hyg. 2012;4(2):12–5. [Google Scholar]
- Baer PN, Lester M. The thumb, the pacifier, the erupting tooth and a beautiful smile. J Pedod. 1987;11:113–9. [PubMed] [Google Scholar]
- Proffit WR, Fields HW. Contemporary Orthodontics. 3rd ed. USA: Mosby; 2000. pp. 129–35. [Google Scholar]
- Warren JJ, Bishara SE, Steinbock KL, Yonezu T, Nowak AJ. Effects of oral habits’ duration on dental characteristics in the primary dentition. J Am Dent Assoc. 2001;132(12):1685–93. [PubMed] [Google Scholar]
- Gale EN, Ayer WA. Thumb-sucking revisited. Am J Orthod. 1969;55(2):167–70. [PubMed] [Google Scholar]
- Yemitan TA, daCosta OO, Sanu OO, Isiekwe MC. Effects of digit sucking on dental arch dimensions in the primary dentition. Afr J Med Med Sci. 2010;39(1):55–61. [PubMed] [Google Scholar]
- Melsen B, Stensgaard K, Pedersen J. Sucking habits and their influence on swallowing pattern and prevalence of malocclusion. Eur J Orthod. 1979;1(4):271–80. [PubMed] [Google Scholar]
- Maguire JA. The evaluation and treatment of pediatric oral habits. Dent Clin North Am. 2000;44(3):659–69. [PubMed] [Google Scholar]
- Sayin MO, Akin E, Karaçay S, Bulakbasi N. Initial effects of the tongue crib on tongue movements during deglutition: A Cine-Magnetic resonance imaging study. Angle Orthod. 2006;76:400–5. [PubMed] [Google Scholar]
- Haryett RD, Hansen FC, Davidson PO, Sandilands ML. Chronic thumb-sucking: The psychologic effects and the relative effectiveness of various methods of treatment. Am J Orthod. 1967;53(8):569–85. [PubMed] [Google Scholar]
- Villa NL, Cisneros GJ. Changes in the dentition secondary to palatal crib therapy in digit-suckers: A preliminary study. Pediatr Dent. 1997;19(5):323–6. [PubMed] [Google Scholar]
- Schwestka-Polly R, Engelke W, Hoch G. Electromagnetic articulography as a method for detecting the influence of spikes on tongue movement. Eur J Orthod. 1995;17(5):411–7. [PubMed] [Google Scholar]
- Premkumar S. Orthodontics Exam Preparatory Manual for Undergraduates. New Delhi, India: Elsevier Health Sciences; 2011. pp. 535–42. [Google Scholar]
- Farsi NM, Salama FS. Sucking habits in Saudi children: Prevalence, contributing factors and effects on the primary dentition. Pediatr Dent. 1997;19(1):28–33. [PubMed] [Google Scholar]
- Linder-Aronson S. Adenoids: their effects on mode of breathing and nasal air flow and their relationship to characteristics of the facial skeleton and the dentition. A biometric, rhino-manometric and cephalometro-radiographic study on children with and without adenoids. Acta Otolaryngol Suppl. 1970;265:1–132. [PubMed] [Google Scholar]
- Linder-Aronson S. Orthodontics in the Swedish Public Dental Health System. Transactions of the European Orthodontic Society. 1974:233–240. [PubMed] [Google Scholar]
- Brin I, Zwilling-Sellan O, Harari D, et al. Does a secular trend exist in the distribution of occlusal patterns? Angle Orthod. 1998;68:81–84. [PubMed] [Google Scholar]
- Vázquez-Nava F, Quezada-Castillo JA, Oviedo-Treviño S, et al. Association between allergic rhinitis, bottle feeding, nonnutritive sucking habits, and malocclusion in the primary dentition. Arch Dis Child. 2006;91:836–840. [PMC free article] [PubMed] [Google Scholar]
- Viggiano D, Fasano D, Monaco G, et al. Breast feeding, bottle feeding and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch Dis Child. 2004;89:1121–1123. [PMC free article] [PubMed] [Google Scholar]
- Larsson E. Artificial sucking habits: Etiology, prevalence and effect on occlusion. Int J Orofacial Myology. 1994;20:10–21. [PubMed] [Google Scholar]
- Larsson E. Sucking, chewing and feeding habits and the development of crossbite: A longitudinal study of girls from birth to 3 years of age. Angle Orthod. 2001;71:116–119. [PubMed] [Google Scholar]
- Warren JJ, Bishara SE, Steinbock KL. Effects of oral habits� duration on dental characteristics in the primary dentition. J Am Dent Assoc. 2001;132:1685–1693. [PubMed] [Google Scholar]
- Castelo PM, Gavião MB, Pereira LJ, et al. Maximal bite force, facial morphology and sucking habits in young children with functional posterior crossbite. J Appl Oral Sci. 2010;18:143–148. [PMC free article] [PubMed] [Google Scholar]
- Melink S, Vagner MV, Hocevar-Boltezar I, et al. Posterior crossbite in the deciduous dentition period, its relation with sucking habits, irregular orofacial functions, and otolaryngological findings. Am J Orthod Dentofacial Orthop. 2010;138:32–40. [PubMed] [Google Scholar]
- Carrascoza KC, Possobon RF, Tomita LM, et al. Consequences of bottle-feeding to the oral facial development of initially breastfed children. J Pediatr Rio J. 2006;82:395–397. [PubMed] [Google Scholar]
- Ovsenik M. Incorrect orofacial functions until 5 years of age and their association with posterior crossbite. Am J Orthod Dentofacial Orthop. 2009;136:375–381. [PubMed] [Google Scholar]
- Warren DW. Effect of airway obstruction upon facial growth. Otolaryngol Clin North Am. 1990;23:699–712. [PubMed] [Google Scholar]
- Harvold EP, Tomer BS, Vargervik K, et al. Primate experiments on oral respiration. Am J Orthod. 1981;79:359–372. [PubMed] [Google Scholar]
- Harari D, Redlich M, Miri S, et al. The effect of mouth breathing versus nasal breathing on dentofacial and craniofacial development in orthodontic patients. Laryngoscope. 2010;120:2089–2093. [PubMed] [Google Scholar]
- Souki BQ, Pimenta GB, Souki MQ, et al. Prevalence of malocclusion among mouth breathing children: do expectations meet reality? Int J Pediatr Otorhinolaryngol. 2009;73:767–773. [PubMed] [Google Scholar]
- Jefferson Y. Mouth breathing: adverse effects on facial growth, health, academics, and behavior. Gen Dent. 2010;58:18–25. [PubMed] [Google Scholar]
- Grippaudo C, Paolantonio EG, Deli R, et al. Validation of the Risk Of Malocclusion Assessment (ROMA) Index. Eur J Paediatr Dent. 2007;8:136–142. [PubMed] [Google Scholar]
- Grippaudo C, Pantanali F, Paolantonio EG, et al. Prevalence of malocclusion in Italian schoolchildren and orthodontic treatment need. Eur J Paediatr Dent. 2013;14:314–318. [PubMed] [Google Scholar]
- Grippaudo C, Pantanali F, Paolantonio EG, et al. Orthodontic treatment timing in growing patients. Eur J Paediatr Dent. 2013;14:231–236. [PubMed] [Google Scholar]
- Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11:309–320. [PubMed] [Google Scholar]
- Garde JB, Suryavanshi RK, Jawale BA, et al. An epidemiological study to know the prevalence of deleterious oral habits among 6 to 12 year old children. J Int Oral Health. 2014;6:39–43. [PMC free article] [PubMed] [Google Scholar]
- Dean JA, McDonald RE, Avery DA. Managing the developing occlusion. St. Louis, Mo: Mosby and Co.; 2000. pp. 178–217. [Google Scholar]
- Graber TM. The ‘three Ms’: muscles, malformation, and malocclusion. Am J Orthod. 1963;49:418–450. [Google Scholar]
- Graber TM, Rakosi T, Petrovic AG. Dentofacial orthopedics with functional appliances. 1st Edition. St. Louis, MO: Mosby; 1985. [Google Scholar]
- Warren JJ, Slayton RL, Bishara SE, et al. Effects of nonnutritive sucking habits on occlusal characteristics in the mixed dentition. Pediatr Dent. 2005;27:445–450. [PubMed] [Google Scholar]
- Telles FBA, Ferreira RI, Magalhães LNC, et al. Effect of breast- and bottle-feeding duration on the age of pacifier use persistence. Braz Oral Res. 2009;23:432–438. [PubMed] [Google Scholar]
- Charchut SW, Allred EN, Needleman HL. The effects of infant feeding patterns on the occlusion of the primary dentition. J Dent Child. 2003;70:197–203. [PubMed] [Google Scholar]
- Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93:149–152. [PubMed] [Google Scholar]
- Graber TM, Chung DDB, Aoba JT. Dentofacial orthopedics versus orthodontics. J Am Dent Assoc. 1969;75:1145–1166. [PubMed] [Google Scholar]
- Demir A, Uysal T, Basciftci FA, et al. The association of occlusal factors with masticatory muscle tenderness in 10- to 19-year old Turkish subjects. Angle Orthod. 2005;75:40–46. [PubMed] [Google Scholar]
- Kayukawa H. Malocclusion and masticatory muscle activity: a comparison of four types of malocclusion. J Clin Pediatr Dent. 1992;16:162–177. [PubMed] [Google Scholar]
- Esteves A, Bommarito S. Evaluation of palatine depth and dimensions of the upper dental arch in patients with malocclusion and different facial types. Rev Dent Press Orthodon Ortop Facial. 2007;12:84–98. [Google Scholar]
- Levrini A. 1989;3 Le abitudini viziate. Quaderni di Odontoiatria Infantile Elsevier. [Google Scholar]
- Cozza P, Baccetti T, Franchi L, et al. Transverse features of subjects with sucking habits and facial hyperdivergency in the mixed dentition. Am J Orthod Dentofacial Orthop. 2007;132:226–229. [PubMed] [Google Scholar]
- Valera FC, Travitzki LV, Mattar SE, et al. Muscular, functional and orthodontic changes in preschool children with enlarged adenoids and tonsils. J Pediatr Otorhinolaringol. 2003;67:761–770. [PubMed] [Google Scholar]
- Skoner DP. Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol. 2001;108:S2–S8. [PubMed] [Google Scholar]
- Bellanti JA, Wallerstedt DB. Allergic rhinitis update: epidemiology and natural history. Allergy Asthma Proc. 2000;21:367–370. [PubMed] [Google Scholar]
- Sousa JB, Anselmo-Lima WT, Valera FC, et al. Cephalometric assessment of the mandibular growth pattern in mouth-breathing children. J Pediatr Otorhinolaryngol. 2005;69:311–317. [PubMed] [Google Scholar]
- Solow B, Kreiborhg S. Soft tissue stretching: a possible control factor in craniofacial morphogenesis. J Dent Res. 1977:505–507. [PubMed] [Google Scholar]
- Rubin RM. Mode of respiration and facial growth. Am J Orthod. 1980;78:504–510. [PubMed] [Google Scholar]
- Mocellin M, Fugmann EA, Gavazzoni FB. Estudo cefalometrico- radiografico e otorrinolaringologico correlacionado o grau de obstrucao nasal e o padrao de crescimento facial em pacientes nao tratados ortodonticamente. Rev Bras Otorrinolaringol. 2000;66:116–120. [Google Scholar]
- Reed E, Kiebach TJ, Martin C, et al. Stability of early class III orthopedic treatment. Semin Orthod. 2014;20:114–127. [Google Scholar]
- Bresolin D, Shapiro PA, Shapiro GG, et al. Mouth breathing in allergic children: Its relationship to dentofacial development. Am J Orthod. 1983;83:334–334. [PubMed] [Google Scholar]
- Bresolin D, Shapiro GG, Shapiro PA, et al. Facial characteristics of children who breathe through the mouth. Pediatrics. 1984;73:622–625. [PubMed] [Google Scholar]
- Trask GM, Shapiro GG, Shapiro PA. The effects of perennial allergic rhinitis on dental and skeletal development: a comparison of sibling pairs. Am J Orthod Dentofacial Orthop. 1987;92:286–293. [PubMed] [Google Scholar]
- Rakosi T, Schilli W. Class III anomalies: a coordinated approach to skeletal, dental, and soft tissue problems. J Oral Surg. 1981;39:860–870. [PubMed] [Google Scholar]
- Vig KW. Nasal obstruction and facial growth: the strength of evidence for clinical assumptions. Am J Orthod Dentofacial Orthop. 1998;113:603–611. [PubMed] [Google Scholar]
- Wagaiyu EG, Ashley FP. Mouth breathing, lip seal and upper lip coverage and their relationship with gingival inflammation in 11-14 year-old schoolchildren. J Clin Periodontol. 1991;18:698–702. [PubMed] [Google Scholar]
- King GJ, Keeling SD, Hocevar RA, et al. The timing of treatment for Class II malocclusions in children: a literature review. Angle Orthod. 1990;60:87–97. [PubMed] [Google Scholar]
- Kluemper GT, Beeman CS, Hicks EP. Early orthodontic treatment: what are the imperatives? J Am Dent Assoc. 2000;131:613–620. [PubMed] [Google Scholar]
- Musich D, Busch MJ. Early orthodontic treatment: current clinical perspectives. Alpha Omegan. 2007;100:17–24. [PubMed] [Google Scholar]