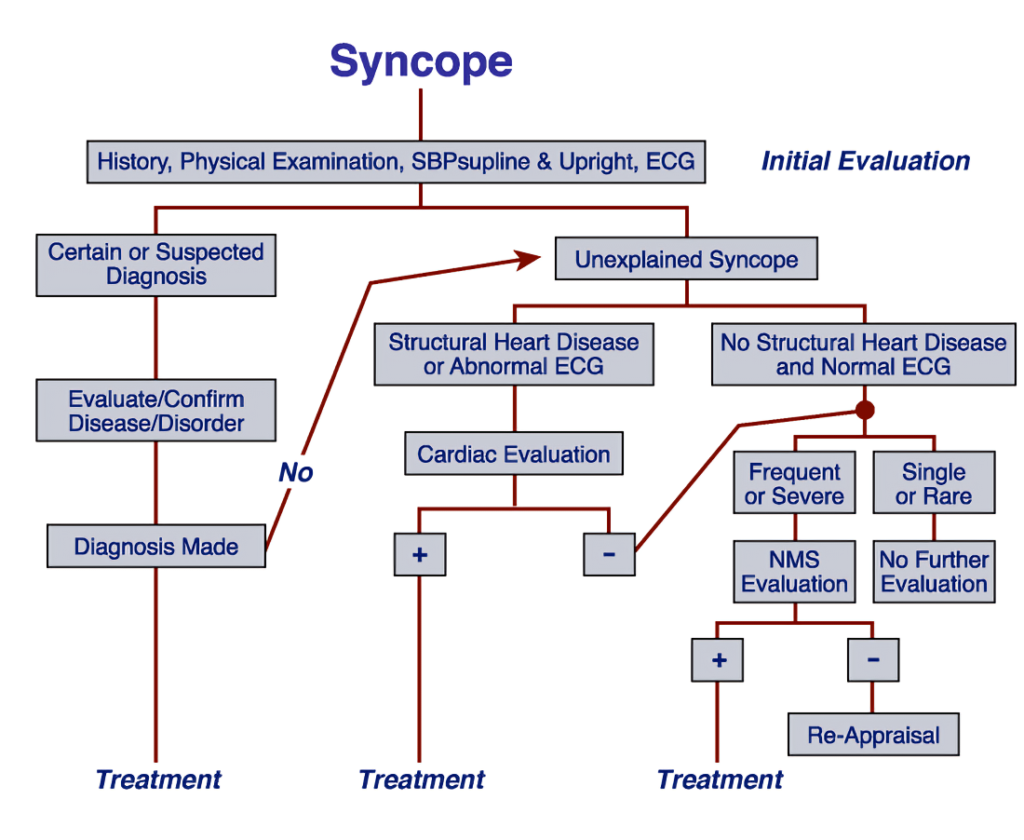
The management of syncope begins with a thorough evaluation by a healthcare professional.
This includes:
Medical History Review: A detailed history of the patient’s episodes, including frequency, duration, triggers (such as standing up quickly or emotional distress), and any associated symptoms (like lightheadedness or palpitations).
Physical Examination: A comprehensive physical exam focusing on cardiovascular and neurological systems.
Cardiovascular Examination includes Heart Sounds: Auscultation should focus on identifying any abnormal heart sounds, murmurs, or signs of congestive heart failure
Vital Signs Monitoring: Blood pressure and heart rate should be measured in various positions (lying down, sitting, standing) to assess for orthostatic hypotension.
Diagnostic Testing
Depending on the initial assessment findings, further diagnostic tests may be warranted:
Electrocardiogram (ECG): to check for arrhythmias or other cardiac abnormalities.
Echocardiogram: To evaluate structural heart issues that could lead to syncope.
Holter Monitor: Continuous monitoring of heart rhythms over 24-48 hours can help identify intermittent arrhythmias.
Tilt Table Test: This test helps diagnose vasovagal syncope by simulating changes in posture and observing blood pressure and heart rate responses.
Neurological Evaluation: If neurologic causes are suspected, imaging studies like CT or MRI may be performed.
Blood Tests: To check for anemia, electrolyte imbalances, or other metabolic issues that could contribute to syncope.
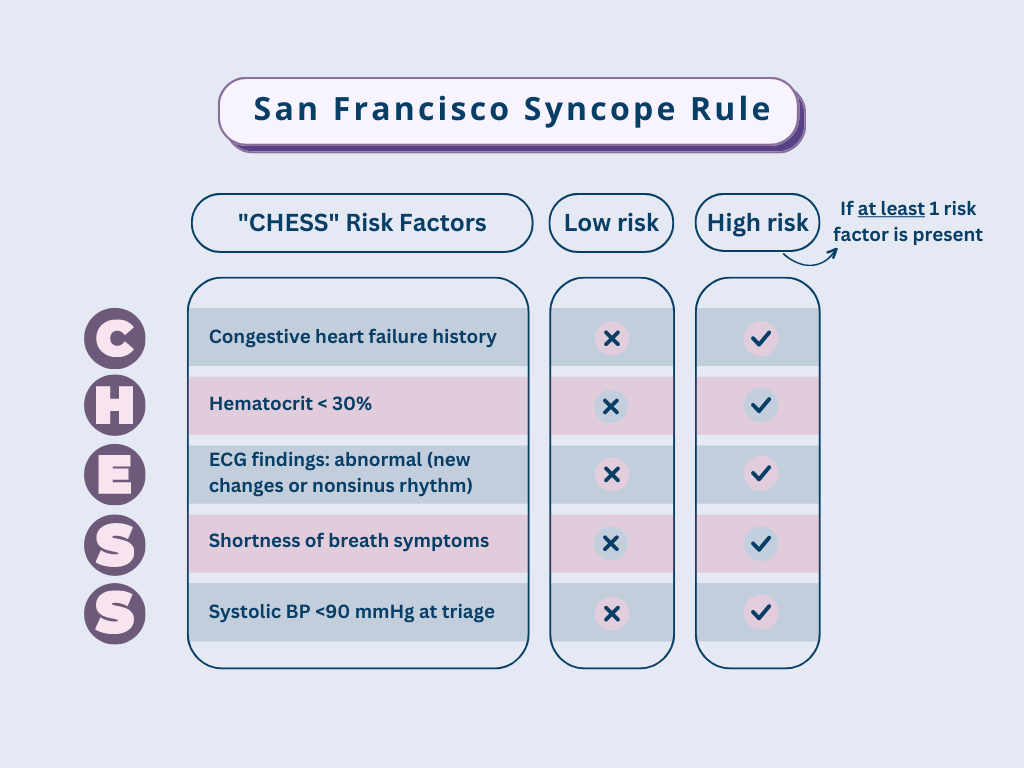
San Francisco Syncope Rule
The San Francisco Syncope Rule (SFSR) is a clinical decision-making tool designed to evaluate the risk of serious outcomes in patients who present with syncope (fainting).
The rule aims to identify patients at high risk for serious outcomes, such as death or significant morbidity, following an episode of syncope.
Criteria of the San Francisco Syncope Rule:
The SFSR uses the mnemonic CHESS to outline five key criteria that indicate a higher risk of serious outcomes:
C – History of Congestive Heart Failure: A past medical history of congestive heart failure increases the likelihood of significant cardiovascular issues following syncope.
H – Hematocrit < 30%: Low hematocrit levels can indicate anemia or other underlying conditions that may contribute to syncope and increase the risk of serious outcomes.
E – Abnormal ECG: Any new changes on an electrocardiogram (ECG), including non-sinus rhythms or other abnormalities, suggest potential cardiac problems that could lead to adverse events.
S – Shortness of Breath: The presence of dyspnea may indicate underlying respiratory or cardiac issues, raising concern for serious complications.
S – Triage Systolic Blood Pressure < 90 mmHg: A low systolic blood pressure at triage suggests hemodynamic instability, which is associated with increased risk for adverse outcomes.
If any one of these criteria is present in a patient who has experienced syncope, they cannot be classified as “low risk” for serious outcomes. Serious outcomes are defined broadly and include:
Death
Myocardial infarction
Arrhythmia
Pulmonary embolism
Stroke
Subarachnoid hemorrhage
Significant hemorrhage
Management of Syncope
Basic management that is recommended for all the patients is:
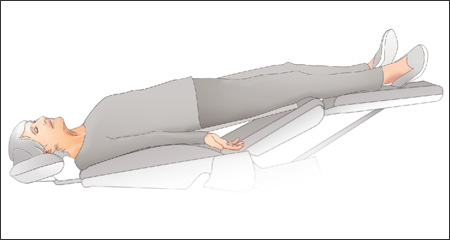
Position
It is the first and most important step in the management of syncope.
The patient should be placed in a supine or anti-trendelenburg position with his or her legs slightly elevated.
This position stops the progression of the symptoms of syncope.
This movement helps in increasing the blood return to the heart from the peripheries.
Circulation
Assessment of Vital Signs: Check for pulse, blood pressure, and signs of shock. A rapid heart rate or low blood pressure may indicate inadequate circulation.
Intravenous (IV) Access: Establishing IV access allows for fluid resuscitation if needed, especially if the patient is hypotensive or dehydrated.
Cardiac Monitoring: Continuous monitoring of heart rhythm is essential, as arrhythmias can be a cause or consequence of syncope.
Pharmacologic Support: In cases where there is significant hypotension or poor perfusion, medications such as vasopressors may be administered to stabilize blood pressure.
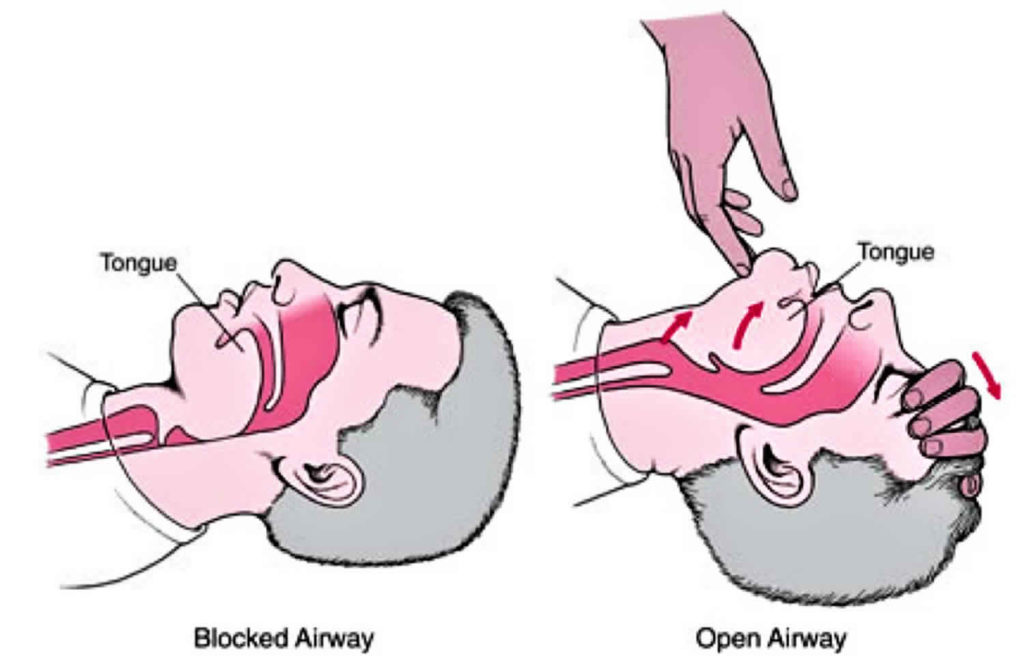
Airway
Maintaining a patent airway is critical during an episode of syncope:
Positioning: If the patient is unconscious but breathing, place them in the recovery position (on their side) to prevent aspiration and maintain an open airway.
Oxygen Administration: Supplemental oxygen may be provided if there are signs of respiratory distress or hypoxia.
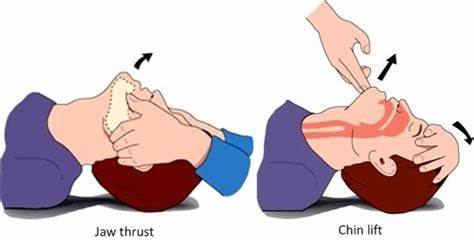
Advanced Airway Techniques: If the patient does not regain consciousness quickly or shows signs of compromised airway protection (e.g., inability to maintain their own airway), advanced airway management techniques may be necessary.
Advanced airway management encompasses a variety of techniques designed to secure and maintain a patent airway in patients who are unable to breathe adequately on their own.
These techniques can be categorized into several groups, each with specific applications, indications, and methods.
1. Intubation Techniques
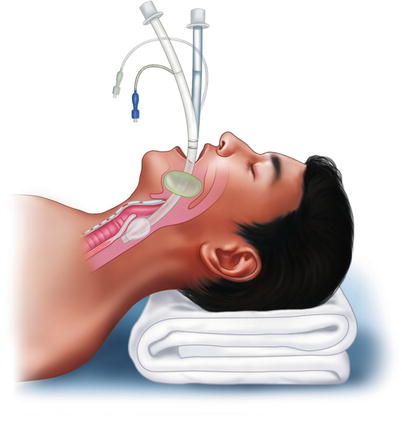
i. Orotracheal Intubation
Definition: The placement of an endotracheal tube (ETT) through the mouth into the trachea.
Indications: Used for patients requiring mechanical ventilation or those at high risk for aspiration.
Procedure: Involves direct laryngoscopy to visualize the vocal cords and guide the ETT into the trachea.
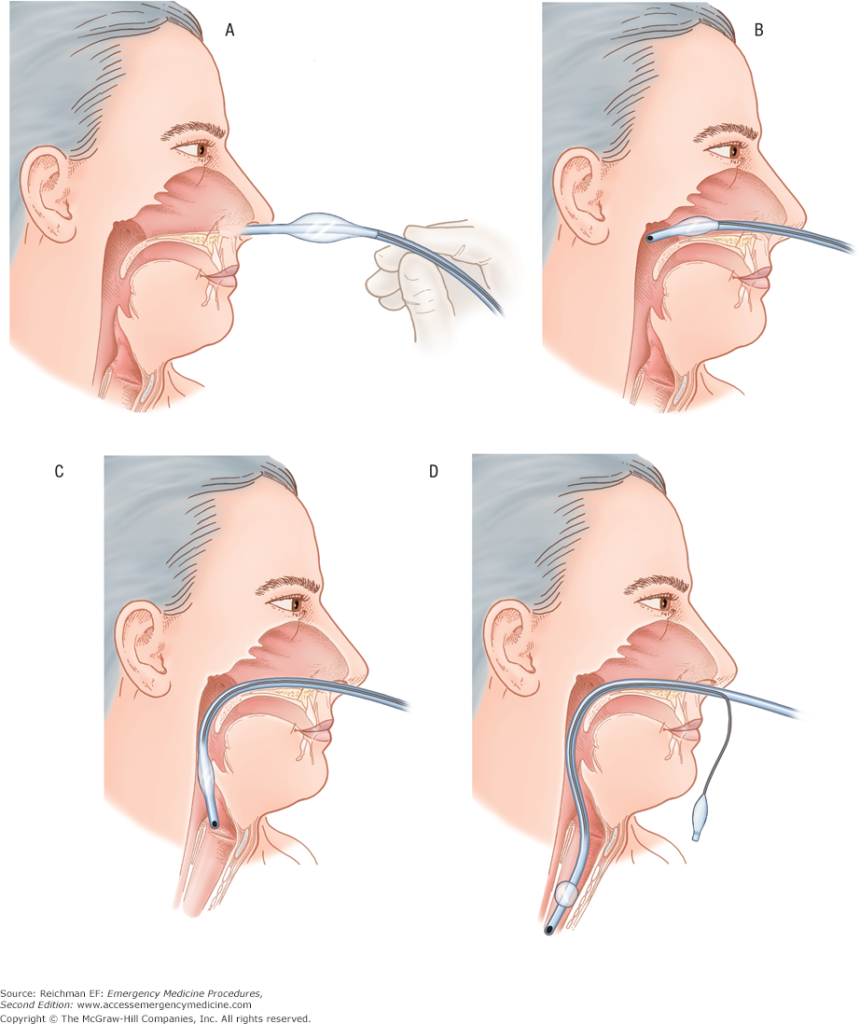
ii. Nasotracheal Intubation
Definition: Insertion of an ETT through the nose into the trachea.
Indications: Suitable for conscious patients with intact gag reflexes who require intubation but have limited mouth opening.
Considerations: Not recommended in cases of suspected skull fractures or significant facial trauma.
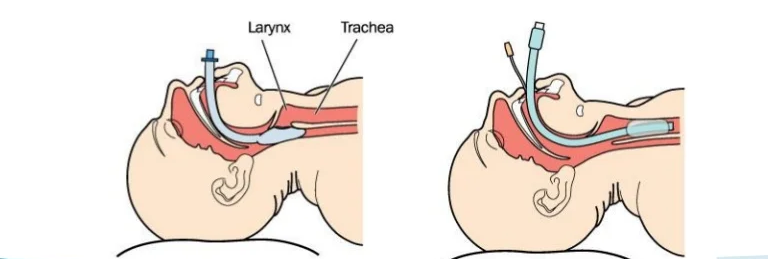
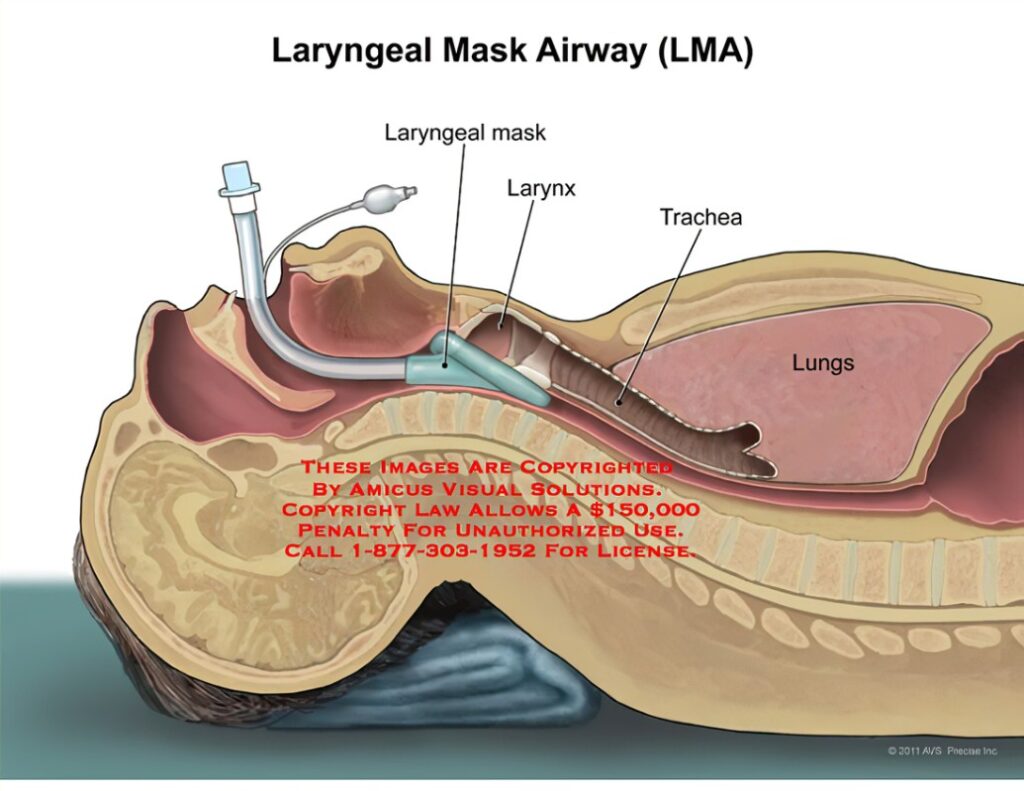
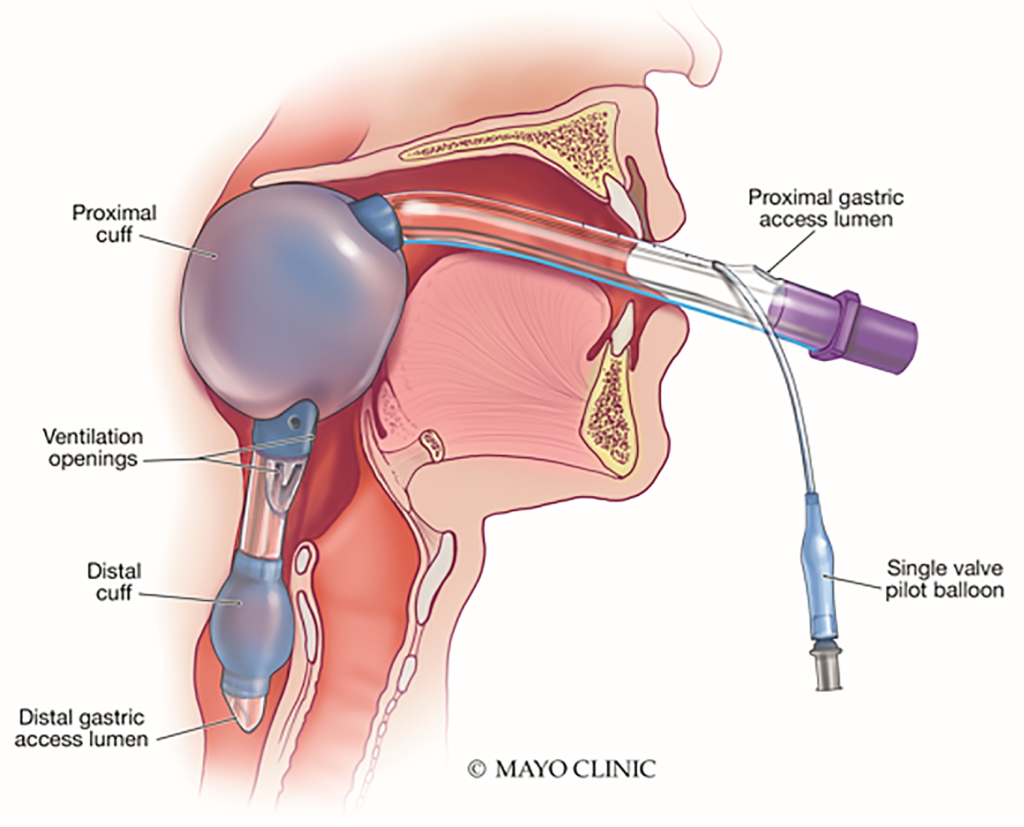
iii. Laryngeal Mask Airway (LMA)
Definition: A supraglottic airway device that sits above the vocal cords.
Indications: Useful in situations where intubation is difficult or when rapid airway control is needed without full anesthesia.
Types: Classic LMA and ProSeal LMA are commonly used, especially in pediatric populations
iv. Blind Insertion Devices
Examples: Combitube and King LT.
Indications: Employed in emergencies when traditional intubation fails; these devices can be inserted without direct visualization of the glottis.
2. Surgical Airways
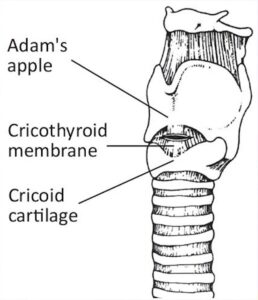
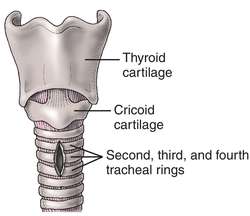
i. Cricothyrotomy
Definition: An emergency procedure involving an incision through the cricothyroid membrane to establish an airway.
Indications: Indicated when other methods fail or are not feasible, particularly in cases of severe airway obstruction.
Advantages: Quicker to perform than a tracheotomy and associated with fewer complications.
ii. Tracheotomy
Definition: A surgical procedure creating an opening directly into the trachea through an incision in the neck.
Indications: Typically performed for long-term ventilation needs or when prolonged airway access is required.
Considerations: More complex than cricothyrotomy and usually done in controlled settings.
Breathing
Assessing and supporting breathing is vital during syncope management:
Respiratory Assessment: Monitor respiratory rate and effort. Look for any signs of respiratory distress or abnormal breath sounds.
Assistance with Ventilation: If the patient exhibits inadequate breathing (e.g., shallow breaths or apnea), bag-mask ventilation may be required until further help arrives or until they regain adequate spontaneous breathing.
Continuous Monitoring: Keep track of oxygen saturation levels using pulse oximetry to ensure that the patient maintains adequate oxygenation throughout their care.
Definitive care
Administration of oxygen: During the episode, oxygen may be administered anytime to the syncopal or post syncopal patient.
Monitoring of vital signs: All the vital signs including blood pressure, respiratory rate and heart rate should be monitored closely.
Respiratory stimulants such as aromatic ammonia may be placed near the patient’s nose to inhale it.
All binding and tight clothes like ties, belts and collars should be loosened up
Drugs Used in Treatment of Syncope
The management of syncope often involves pharmacotherapy aimed at preventing episodes and reducing morbidity.
Here are some drugs commonly used:
Fludrocortisone: This medication helps increase blood volume and improve blood pressure, particularly useful in cases of orthostatic hypotension.
Midodrine: An alpha-agonist that increases blood pressure by constricting blood vessels, effective for patients with orthostatic hypotension.
Ephedrine: Although this drug can be used to treat vasodepressor carotid sinus syndrome, it has limitations due to side effects.
Dihydroergotamine: Effective for vasodepressor carotid sinus syndrome but poorly tolerated long-term due to side effects.
Serotonin antagonists (e.g., fluoxetine, sertraline): These have been reported as potentially effective in managing vasovagal syncope, although further clinical trials are needed to validate their use.
Dental Considerations
Syncope is one of the most common medical emergencies encountered in dental offices.
Studies indicate that it accounts for approximately 50% of all medical emergencies reported by dentists.
The condition can occur in patients of all ages but is particularly prevalent among young adults and those with a history of anxiety related to dental treatment.
Risk Factors
Several risk factors contribute to the likelihood of syncope occurring during dental procedures:
Psychogenic factors: anxiety, fear of dental treatment, and emotional stress are significant triggers. Patients with a history of negative experiences in dental settings are at higher risk.
Physical factors: prolonged standing or sitting in an upright position can lead to blood pooling in the extremities, decreasing cerebral perfusion. Other physical contributors include dehydration, hunger, exhaustion, and hot environments.
Medical History: A thorough medical history should be taken to identify any predisposing conditions, such as cardiovascular issues or previous episodes of syncope.
Signs and Symptoms
The signs preceding syncope can be divided into early and late stages:
Early Signs: Feelings of warmth, pallor (ashen-grey skin), excessive sweating (diaphoresis), nausea, slight hypotension (low blood pressure), and tachycardia (increased heart rate).
Late Signs: pupillary dilation, yawning, cold extremities, significant hypotension, bradycardia (decreased heart rate), visual disturbances, dizziness, and eventual loss of consciousness.
Emergency Management Protocols
If a patient experiences syncope during a dental procedure:
Discontinue Treatment: Immediately stop any ongoing procedures.
Positioning: Place the patient in a supine position with their legs elevated slightly (Trendelenburg position) to promote venous return.
Assess Vital Signs: Monitor airway patency and circulation; check pulse and blood pressure.
Oxygen Administration: Provide supplemental oxygen to enhance cerebral perfusion.
Stimulation Techniques: Use aromatic ammonia inhalants if necessary to stimulate consciousness through irritant fumes.
Post-Syncopal Care: If recovery occurs within 15 minutes, postpone further treatment; if not recovered after 15 minutes or if vital signs deteriorate, activate emergency medical services (EMS).
Preventive Measures
To minimize the risk of syncope during dental visits:
Conduct thorough medical histories to identify at-risk patients.
Advise anxious patients to eat lightly before appointments to maintain stable glucose levels.
Utilize techniques such as nitrous oxide sedation for anxiety management.
Ensure that patients are treated in a reclined position whenever possible.
By understanding these considerations regarding syncope in dental practices—its causes, symptoms, emergency responses, and preventive measures—dental professionals can better prepare for potential emergencies and ensure patient safety. [9]
CONCLUSION
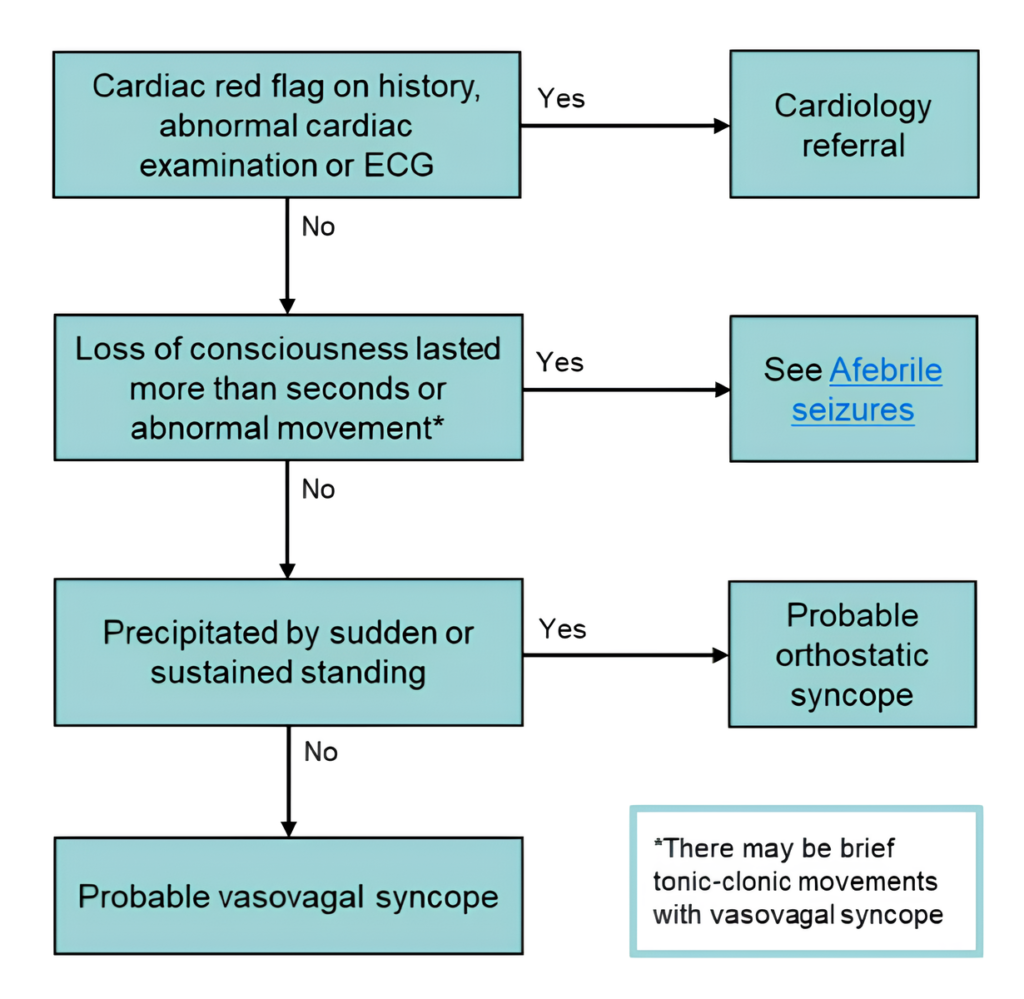
In summary, syncope is a transient loss of consciousness characterized by an inability to maintain postural tone, followed by spontaneous recovery.
It can arise from various etiologies, broadly categorized into reflex (neurally mediated), orthostatic, and cardiac causes.
While many instances of syncope are benign and often related to situational or vasovagal triggers, it is crucial to recognize that some cases may indicate serious underlying conditions that could lead to increased morbidity or mortality.
The evaluation of syncope should begin with a thorough history and physical examination, focussing on the circumstances surrounding the event, associated symptoms, and any potential risk factors.
Diagnostic testing, including ECG and possibly imaging studies or prolonged monitoring, may be necessary to identify the underlying cause.
Management strategies will vary based on the etiology but often include patient education and lifestyle modifications for benign causes or more intensive interventions such as medication or device therapy for cardiac-related syncope.
Ultimately, understanding the multifaceted nature of syncope is essential for effective diagnosis and management.
Clinicians must remain vigilant in assessing patients with syncope to differentiate between benign episodes and those requiring urgent intervention.
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
DisagreeAgree
Connect with
I allow to create an account
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
DisagreeAgree
0 Comments
Oldest
NewestMost Voted
Inline Feedbacks
View all comments
Written By
Dr. Ritwik Bishnoi (BDS)
Dr. Ritwik Bishnoi is an India-based board-certified general dentist.